Carcinoma in situ (Tis) refers to cancer that is confined to the gastric ducts and has not yet extended beyond them; early gastric cancer (stage T1a) refers to cancerous tissue confined to the innermost layer of the gastric mucosal layer of the gastric wall, regardless of size or the presence of lymph node metastases.
The treatment of these two types of gastric cancer is similar, and doctors usually follow the following process for diagnosis and treatment: refinement of relevant tests; determination of surgical plan and surgery; postoperative treatment; and follow-up.
Refinement of tests
When gastric cancer is suspected, doctors usually perform gastroscopy and clamp biopsies for pathology, and endoscopic biopsy is now the gold standard for diagnosing gastric cancer. Ultrasound endoscopy and abdominal CT are complementary to plain gastroscopy and can help the physician determine the depth of tumor infiltration and metastases in the perigastric lymph nodes. In addition, patients routinely undergo routine blood tests, blood biochemistry, and tumor markers.
Determine surgical plan and perform surgery
After these examinations, depending on the presence or absence of lymph node metastases and the patient’s wishes, the surgeon will determine which option to use to remove the gastric cancer, either endoscopically with gastrectomy, or laparoscopically or surgically.
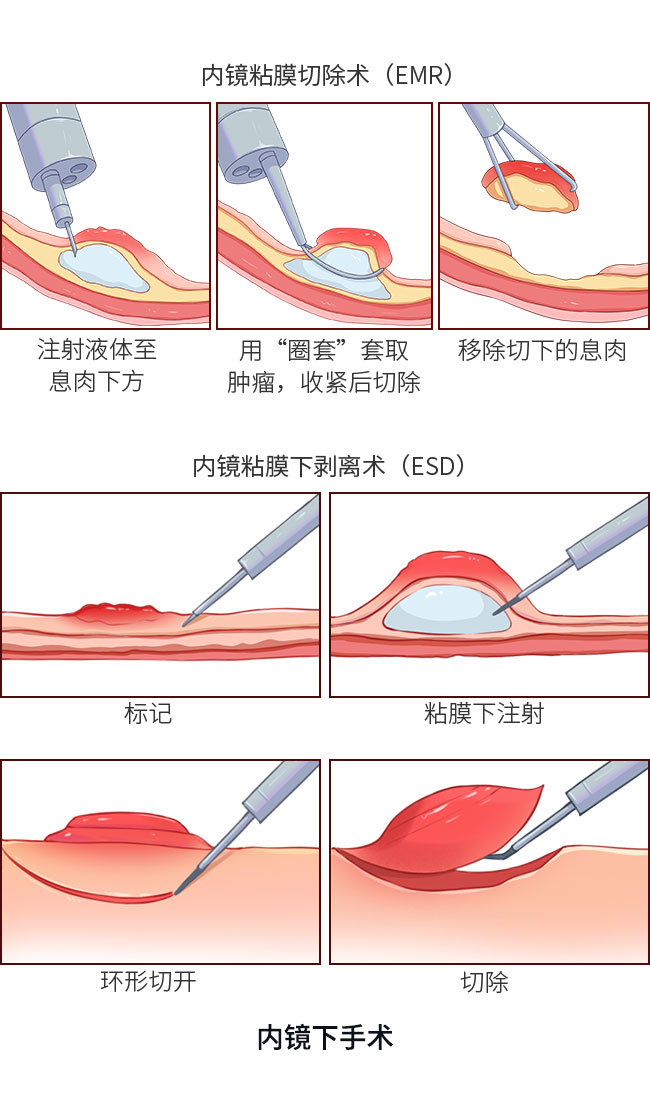
For carcinoma in situ and early gastric cancer without lymph node metastases, if the patient is eligible for endoscopic resection and there are no contraindications, the surgeon will usually recommend endoscopic resection, including endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD), which is an extended resection of the diseased mucosa with a miniature trap or electric knife under direct gastroscopic view.
For patients who are not suitable for endoscopic resection and those who are suspected of having lymph node metastasis, physicians usually perform radical gastric cancer surgery plus lymph node dissection either laparoscopically or surgically for the purpose of radical treatment. Depending on the size and location of the lesion, the extent of tissue removed by the surgeon varies, as does the approach taken to reconstruct the GI tract.
Postoperative treatment
For patients treated with endoscopic resection of gastric cancer, postoperative acid suppressants and gastric mucosal protectors are usually required because of the tendency of the lesion to form ulcers. Prophylactic antibiotics are considered if the preoperative evaluation is extensive for resection, if the operation is prolonged, or if it may cause perforation of the GI tract. For patients who test positive for Helicobacter pylori (Hp), anti-Hp drugs are also commonly used to eradicate Hp and reduce the risk of recurrence.
Patients with carcinoma in situ and early gastric cancer without lymph node metastasis generally do not need adjuvant therapy such as chemotherapy or radiotherapy after surgery.
Patients with early gastric cancer with lymph node metastasis generally need to receive postoperative adjuvant therapy such as chemotherapy or radiotherapy after surgery to reduce the risk of recurrence.
Follow-up visits
The primary goal of follow-up is to detect recurrence and metastasis in a timely manner and to provide treatment to improve overall survival and improve quality of life for patients. Patients with in situ and early-stage gastric cancer treated radically usually require follow-up every 6 months for 3 years after surgery and annually thereafter. The follow-up visit requires a detailed medical history to the physician, who will usually perform a physical examination, blood tests (including tumor markers, etc.), and functional status score. Patients usually have a gastroscopy and a CT scan of the chest and abdomen once a year.
Summary
- In situ and early gastric cancer have a better outcome, and treatment aims to eradicate the tumor and prevent recurrence.
- Surgical resection is the basic treatment for gastric cancer, and doctors usually use minimally invasive treatment to ensure radical tumor cure. After surgery, patients may receive a combination of treatments to reduce the risk of recurrence.
- Physicians will develop an individualized treatment strategy based on factors such as the patient’s disease status and the presence of other diseases. Following the physician’s recommendations for standardized treatment and follow-up after surgery is conducive to a favorable outcome. (Contributed by Songcheng Yin, Department of Gastrointestinal Oncology, The First Hospital of China Medical University)