Gastroscopy is a relatively common test, but many people are still wary of it. In fact, gastroscopy is not as scary as you might think. In this article, we will unravel the “mystery” of gastroscopy and take you through the process of gastroscopy and what to look for.
How does a gastroscopy work?
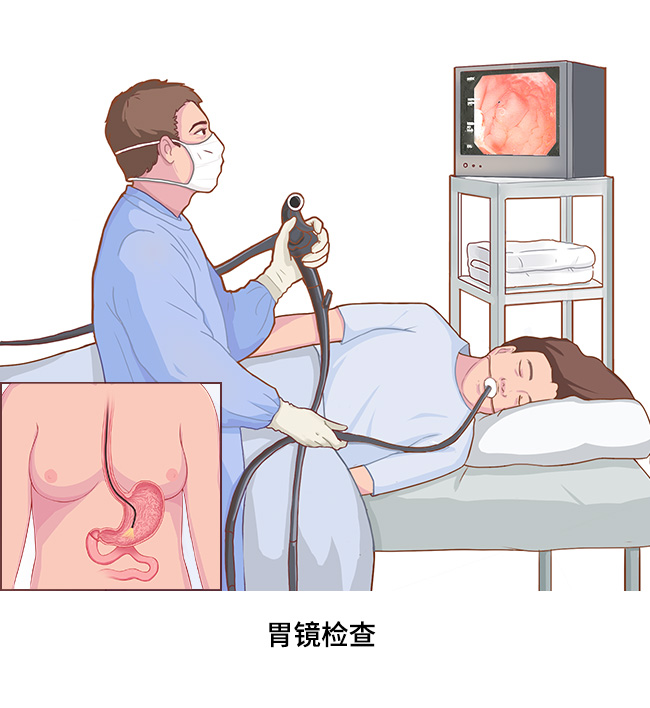
The gastroscopy procedure is a very simple procedure.
The patient is first placed in the following position for the examination, and this position is maintained as much as possible during the examination according to the physician’s request: lying on the left side with the legs bent at the knees and slightly tucked toward the abdomen (legs flexed), with a low pillow under the head and a relaxed neck. The patient needs to loosen the collar and belt, and remove dentures if present.
Usually a gastroscopy is performed using pharyngeal anesthesia (except for painless gastroscopy), where the patient is asked to take a moderate amount of Lidocaine Mucilage deep in the throat for 1 to 2 minutes and then spit it out, or a spray of Lidocaine in the mouth, which is taken in the throat for 30 seconds and spit out. The physician may also give the subject an intramuscular antispasmodic drug or a drug that dissolves mucus in the stomach, as appropriate.
The examinee is asked to hold a mouth cushion and gently bite down on it, and then a long, thin gastroscope “tube” is slowly inserted into the mouth, with the examinee swallowing as the gastroscope reaches the base of the tongue, allowing the gastroscope to pass through the pharynx into the esophagus.
The “path” of the gastroscope through the body is the cardia, fundus, body cavity, sinus, pylorus, duodenum bulb, duodenum descending, and papilla, with the doctor retreating to the most distal part to look at each of these areas and check for lesions. 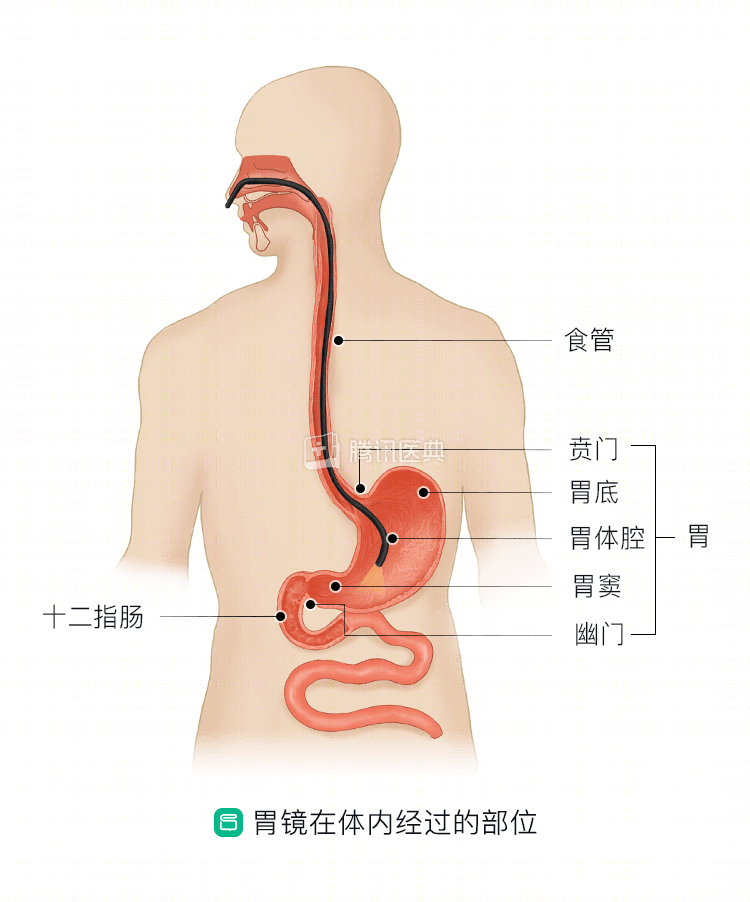
What are the possible risks of gastroscopy?
Gastroscopy may carry the following risks: allergic reactions, with anaphylaxis in severe cases; throat injury, infection, aspiration pneumonia; esophageal cardia tear; esophageal and gastrointestinal perforation; bleeding, which may induce hemorrhage in those with pre-existing esophagogastric varices; induction of severe cardiac arrhythmias; acute myocardial infarction; cerebrovascular disease; and dislocation of the jaw joint.
In the event of a complication during gastroscopy, the physician will usually terminate the examination and manage it immediately. In case of complications related to aspiration, tracheal intubation, opening of the airway, and use of ventilator-assisted breathing are usually performed immediately. For serious surgical complications such as esophageal cardia tears and gastrointestinal perforation, immediate surgical treatment is usually required.
How should I cooperate during the examination?
The patient needs to be positioned as requested by the physician before and during the examination. When inserting the mirror, follow the doctor’s instructions, relax the throat, relax the neck, shoulders, and muscles of the body, breathe in through the nose and out through the mouth, and breathe slowly and deeply.
The key to relaxation is to gently bite down on the mouth pad and accept the gastroscope tube to slide easily through the pharynx, or gently swallow at the doctor’s command, and the slim, smooth gastroscope tube will enter the esophagus smoothly. The subject may experience nausea as the gastroscope passes through the pharynx, may feel a slight pain when it reaches the duodenum, and may feel a tug when a biopsy is taken.
The gastroscopy takes about 10 minutes to complete and may take 20 to 30 minutes for a biopsy. After the gastroscope is inserted, the patient’s body and head should not be turned to prevent damage to the mirror and injury to internal organs. If you feel any discomfort and cannot tolerate it, you can signal the doctor or nurse with hand signals so that the necessary measures can be taken. If you feel uncomfortable during the gastroscopy, inform the doctor in time.
What are the precautions to take after the examination?
- After the examination, the patient should spit out saliva. Because some air enters during the examination, it is normal to experience significant bloating and more belching (i.e., hiccups) at times, although the doctor will suction out the gas when retiring the scope.
- A foreign body sensation, painful discomfort, or a small amount of blood in the saliva may occur in the pharynx after the examination, but there is no need to be alarmed at this time, and do not deliberately vomit or cough. This is due to the damaged pharyngeal mucosa friction during the process of pharyngeal anesthesia and entering the mirror, and deliberate vomiting and coughing will lead to increased bleeding.
- Because the anesthesia has not worn off, premature eating tends to allow food to enter the trachea, so the subject should not eat water until after the examination 1 hour. If a pathological examination is performed (the physician will advise), food should be started 2 hours after the examination, and warm, cool, semi-liquid or soft food should be eaten within 1 day after the examination. Avoid eating raw, cold, hard and irritating foods, smoking, drinking alcohol, strong tea and coffee after the examination to avoid inducing bleeding from the wound. The examinee must pay attention to whether there is black stool (i.e., stool is tarry or asphalt-like, which is a manifestation of upper gastrointestinal bleeding), and should contact the doctor promptly if there is black stool.
- If you have severe abdominal pain and vomiting blood or blood in the stool that does not stop after the examination, you should be seen quickly in the emergency room.
- For 1 to 4 days after the test, the patient may feel discomfort or pain in the throat, but it usually does not interfere with eating and daily tasks. Those with more severe symptoms may rest and should not drive alone the day after the examination. It is best to have a family member accompany you for the gastroscopy and escort you home at the end of the examination.
.
Understand the above gastroscopy procedure and precautions, follow the doctor’s instructions to prepare, cooperate during the examination, and remember and follow some precautions after the examination, it is believed that patients who undergo gastroscopy will no longer be “scared” of it. (Written by Yu Miao, Department of Gastrointestinal Oncology, First Affiliated Hospital of China Medical University)