A young engineer, Xiao Wang, was found to have a 7 cm diameter tumor in his left kidney by B-ultrasound during a health checkup organized by his unit, and the doctor in charge of the checkup recommended that he go to a large hospital to confirm the diagnosis. Xiao Wang came to the urology department of a large hospital with a nervous mood and underwent B-ultrasound, routine blood tests, urinalysis, liver and kidney function tests, enhanced CT, etc., and was finally diagnosed with kidney cancer. But Xiao Wang still could not help but doubt, “Is the diagnosis accurate? Could it be a misdiagnosis? The company’s main goal is to provide the best possible service to its customers.
So what tests are needed to confirm a diagnosis of kidney cancer?
Diagnosis of kidney cancer relies mainly on imaging tests
Currently, medical imaging is the main way to detect or diagnose kidney cancer, including:
- Abdominal B-ultrasound or color Doppler ultrasound (color ultrasound for short) examinations;
- electronic computed tomography (CT);
- magnetic resonance imaging (MRI);
- positron emission computed tomography (PET) or PET-CT.
- Positron emission computed tomography (PET) or PET-CT.
Based on what is seen on imaging, the doctor can make a preliminary determination of whether the kidney tumor is benign or malignant to decide whether to treat it surgically.
Among these imaging modalities, the easiest and simplest way to diagnose kidney cancer is with B ultrasound, which, although not as accurate as CT, MRI, PET, or PET-CT, is good for simple primary screening to help detect kidney cancer early.
B ultrasound, color ultrasound, CT, and MRI are all commonly used to diagnose kidney cancer, and doctors usually start with a B ultrasound or color ultrasound. If an abnormality is found, CT is performed to confirm it; if CT is still unable to determine the nature of the tumor, or if CT reveals an associated inferior vena cava thrombosis, or if the patient has renal insufficiency, MRI is needed.
PET or PET-CT
PET or PET-CT is expensive and is not more accurate than CT or MRI in diagnosing kidney cancer, so it is less commonly used for kidney cancer diagnosis, but it has some advantages in detecting distant metastases.
In addition, doctors may recommend the following imaging tests depending on the situation:
- Chest x-ray or CT: to determine the presence of lung metastases.
- CT/MRI of the head: to determine if there are brain metastases.
- Nuclear nephrography or intravenous urography ( intravenous urogram, IVU): For patients who cannot have CT-enhanced scans to help determine the status of kidney function.
- Nuclear bone scan (ECT): To detect bone lesions or bone metastases.
Laboratory tests are mainly used for preoperative evaluation and prognosis
There are no specific tumor markers for kidney cancer, so blood tests cannot be used to determine kidney cancer. However, blood tests can be used to understand the patient’s general condition, liver and kidney function, and help doctors determine the patient’s prognosis.
For example, testing blood levels of urea nitrogen and creatinine can give an idea of kidney function, while testing for abnormalities in liver function, complete blood count, hemoglobin, blood calcium, blood glucose, sedimentation, alkaline phosphatase and lactate dehydrogenase, as well as changes before and after treatment, can help doctors determine the effectiveness of treatment.
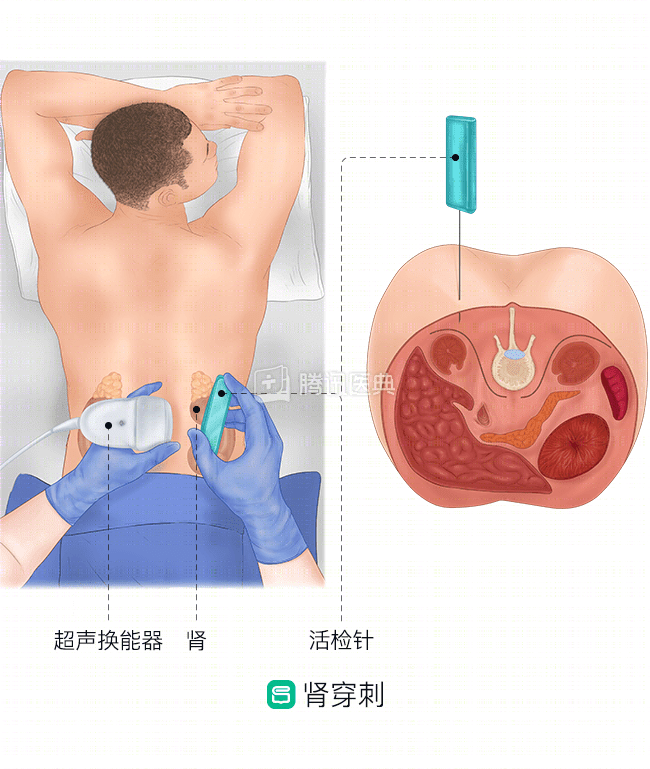
Renal puncture biopsy helps clarify pathologic diagnosis but is not necessary for surgical patients
While pathology is the gold standard for tumor diagnosis, renal aspiration biopsy has limited diagnostic value for kidney cancer. Doctors can usually accurately determine kidney cancer and decide whether to operate based on imaging findings, and for patients who are about to undergo surgery, there is no need for additional renal tumor aspiration biopsy because the resected tumor specimen can be sent directly for testing after surgery.
Renal puncture biopsy is used in the following situations:
- Patients with small renal tumors who have chosen not to treat them for the time being, but to take active monitoring to observe tumor progression;
- Patients who are too old and frail to have surgery;
- Patients who are inoperable and choose instead to undergo radiofrequency ablation, cryoablation, targeted therapy, or radiotherapy.
Patients with the above conditions may opt for a renal puncture biopsy to clarify the diagnosis and guide treatment.
Later ……
Wang was finally unsure and went to another tertiary hospital to confirm the diagnosis and underwent the same tests – ultrasound, CT, blood tests …… The doctor informed him that the kidney tumor was large and should be operated immediately. So Xiao Wang underwent a total excision of his left kidney, and the pathological examination report of the tumor specimen after surgery showed that it was renal clear cell carcinoma, which is one of the most common types of kidney cancer. At present, Xiao Wang is recovering well.
However, sometimes Wang is also afraid that if it were not for his unit’s physical examination, the tumor would have been detected through B-ultrasound in time, and he would not have known how long it would have taken for the diagnosis to be confirmed, and the tumor cells would have been silent and undetectable.