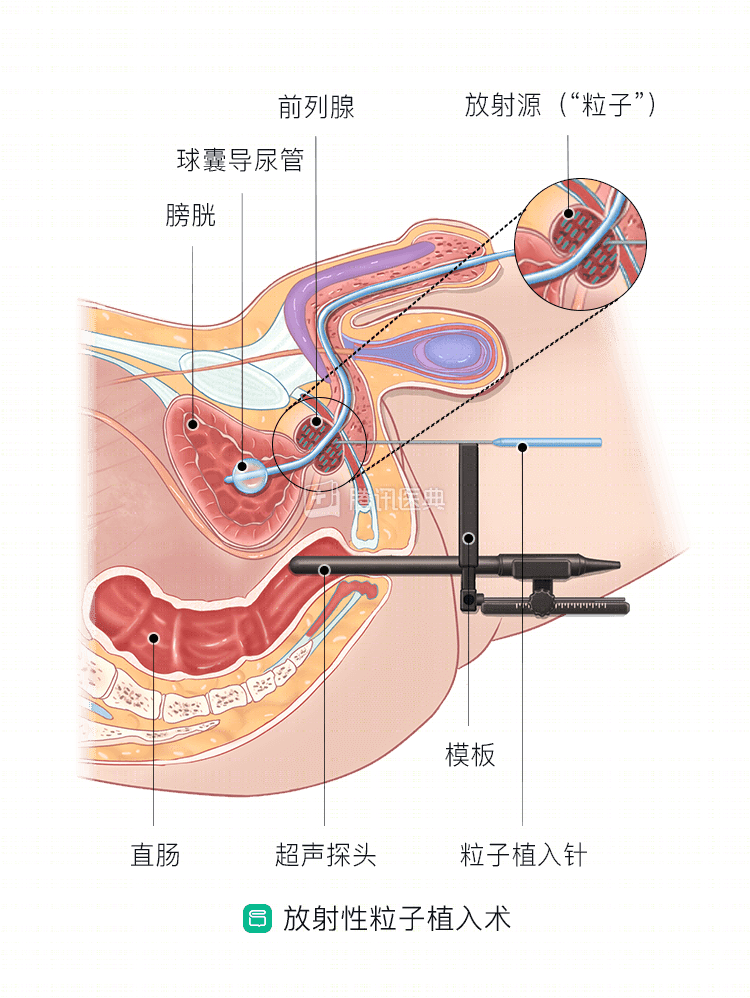
Radiation particle implantation is an important treatment for brachytherapy, in which radioactive particles are positioned inside the prostate through a specific 3D planning system to increase the local radiation dose to the prostate to kill or inhibit prostate cancer cells.
This internal radiation therapy allows the prostate to receive up to two times the radiation dose of external radiation therapy.
Radiation particles commonly used for prostate cancer include:
- I (iodine-125)
- Pd (palladium-103)
- Cs (cesium-131)
Radiation particle implantation has the advantages of minimal invasiveness, good efficacy, few complications, short hospitalization days, and quick recovery.
Which patients are suitable for particle implantation?
In general, particle implantation is a good option.
In general, particle implantation is suitable for patients with all stages of prostate, mainly for limited early stage prostate cancer, but also for intermediate and advanced stage prostate cancer in combination with adjuvant endocrine therapy or external radiation therapy.
Particle implantation for single prostate cancer is only indicated for patients who can be treated with particle implantation to cover all tumor lesions for radical treatment.
Which patients are not candidates for particle implantation?
Patients who are
Particle implantation is an absolute contraindication in patients who meet the following criteria:
- Projected survival less than 5 years;
- Large defects or poor prognosis after electroporation of the prostate;
- Poor general condition, unable to tolerate puncture under local anesthesia;
- With extensive distant metastases.
Particle implantation should be used with caution and is a relative contraindication in patients who meet the following conditions:
- Prostate gland volume greater than 60 ml;
- Previous history of electrodesection of the prostate (small prostate defect and still regular overall morphology);
- Severe diabetes mellitus (need to control blood glucose below 10 mmol/L);
- History of multiple pelvic radiotherapy and surgery.
What is the procedure for particle implantation?
Before implantation, the physiatrist and clinician communicate fully to tune the computerized planning system to each patient and set the relevant parameters, such as radiation dose, spatial resolution, grayscale contrast, geometric precision, and distance measurement. Transrectal ultrasound (TRUS), CT, and MRI can be used to assist in the design of the treatment plan.
What are the considerations after particle implantation?
- Immediately after particle implantation, the surgeon will perform a cystoscopy to remove blood clots and particles that were mistakenly placed in the bladder and urethra, and explain to the patient that there is a risk of particle migration to the lungs or other organs.
- After the particles are implanted, the physician performs a dose distribution analysis, which is used to understand how far the actual treatment has fallen from the initial treatment plan. Although the number of implanted particles can be accurately counted from plain X-rays, plain films alone are not sufficient for post-implantation dose distribution analysis; CT- or MRI-based imaging must be used to assess the distribution of particles within the prostate and the relationship of the particles to the bladder and rectum.
- Regular follow-up of PSA changes and timely adjustment of treatment strategy. The PSA does not drop to very low or even undetectable levels immediately after radioactive particle therapy, but decreases gradually. Typically, it decreases month by month during the first year and plateaus in the second year. Remedial endocrine therapy is promptly administered, especially for intermediate to high-risk patients who experience biochemical relapse.
- The prostate volume does not decrease immediately after radioactive particle therapy, mainly related to post-treatment prostate edema.
- Short-term complications (occurring within 1 year) include, among others.
- Urinary irritation such as urinary frequency, urgency and painful urination;
- Difficulty in urination and increased nocturia;
- Symptoms of rectal irritation such as increased frequency of stool and urgency;
- Proctitis.
These symptoms can be relieved by antispasmodic, analgesic, perineal icing, and stool softening measures.
- Long-term complications (occurring after 1 year) include, among others.
- Chronic urinary retention
- Urethral stricture
- Urinary incontinence
The overall incidence of long-term complications is low.
In conclusion, transperineal prostate cancer radioactive particle implantation is an effective treatment for prostate cancer that is relatively safe and effective, but is complex and highly specialized, requiring close collaboration between radiation oncologists and other specialties for successful completion.
Common confusion and answers
1. Do radioactive particles translocate to other sites?
Particle drift (also known as seed source shift) is possible, but the probability is low. Tapen et al. reported a 5. 9% incidence of seed-borne blood travel to the lung in 290 patients, but none were clinically symptomatic. Immediately after implantation, the surgeon will perform a cystoscopy to remove the displaced particles.
2. Are radioactive particles in the body radiating to family members?
.
Theoretically, although the implanted particles are radioactive, the range of this radioactivity is limited to 2-4 mm, and most of the radiation emitted by the particles is absorbed by the prostate, so patients treated with radioactive particle implants are not radioactive.
In clinical practice, we still recommend that patients be isolated inside the ward and sleep in a single room after implantation. The most important thing is to avoid close and prolonged contact with children or pregnant women at home.
3. Is it possible to have a second implant if the PSA does not decrease significantly?
.
Secondary particle implantation is generally not recommended. If the PSA does not decrease satisfactorily, other treatment options such as combined endocrine or chemotherapy are needed.
Related Questions and Answers: