For some concerns about gastroscopy, many patients ask, “Is it possible to diagnose gastric cancer without a gastroscopy?” and the answer is “no.”
There is no substitute for a gastroscopy to see the lesion and take a biopsy
.
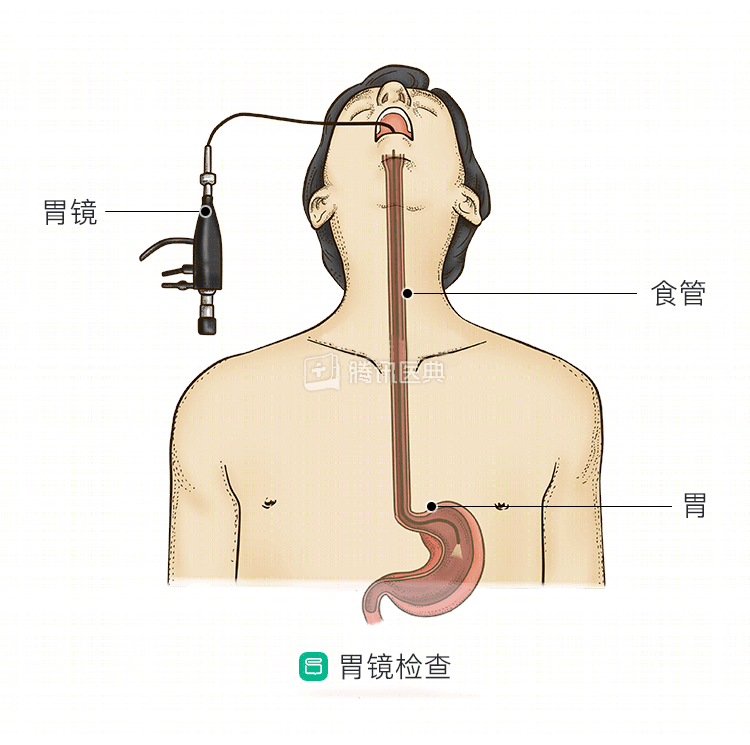
Gastroscopy is like the examiner going into the patient’s stomach, replacing the examiner’s eyes with a realistic view of the lesion that cannot be seen with the naked eye. The gastroscope enters through the mouth and provides a clear view of the mucosa of the esophagus, stomach, duodenum bulb and descending portion. Gastroscopy can not only directly observe the ulcers, polyps, masses and other lesions in these areas, but also take biopsies for pathological examination, which makes gastroscopy play an irreplaceable role in the diagnosis and treatment of gastric cancer. Obtaining a clear pathological diagnosis of gastric cancer is the gold standard that guides doctors in the next step of treatment.
Gastroscopy has outstanding advantages over many tests
The following tests are all more or less deficient compared to gastroscopy:
- Upper gastrointestinal angiography diagnoses gastric cancer by looking at changes in the mucosa, the peristaltic nature of the stomach wall. However, the limitation of upper gastrointestinal angiography is that it can only observe the changes of the gastric wall at the mucosal surface and cannot further reflect the depth of tumor infiltration, the surrounding important lymph nodes and adjacent organs, and also cannot accurately determine early gastric cancer.
- Multi-layer spiral CT has a high soft tissue resolution and can clearly show the perigastric lymph nodes and abdominal lymph nodes. However, CT lacks uniform criteria for diagnosing lymph node metastases, and some lymph nodes may be small in diameter but may have micrometastases; some lymph nodes may be enlarged but may be caused by surrounding inflammation or fibrous reaction.
- Magnetic resonance imaging (MRI) Gastrointestinal peristalsis can cause artifacts on MRI, so it is more constrained in gastrointestinal examinations. To screen for metastases in other organs, physicians recommend MRI for further definitive diagnosis only if the lesion cannot be clearly identified by CT or if the patient is allergic to CT-enhanced contrast agents.
- Positron emission computed tomography (PET-CT) is not widely used for the diagnosis of gastric cancer because of its high cost and radiation exposure.
- Serum tumor marker testing This method is simple, noninvasive, and easily accepted by patients, and is extremely widely used in clinical practice. However, due to the complexity of tumor genes, no tumor has a single type of associated antigen; therefore, the organ specificity of a single tumor marker is limited, and accurate judgments of tumors cannot yet be made on this basis. Currently, there are many serum gastric cancer markers applied in the clinic, but the sensitivity and specificity are not ideal.
Long-chain noncoding RNA has been hotly studied in epigenetic research over the last decade, but accurate assays and clear clinical implications have not yet been available, leading to its inability to be used in the clinic. Moreover, as with other tumor markers, balancing sensitivity and accuracy is the biggest challenge. We can only look forward to future research to further explore its clinical value and clinical application methods.
In conclusion, among the available tests, other tests may be more “comfortable” than gastroscopy, but gastroscopy is the most intuitive, effective, and most importantly, it allows biopsies to be taken for pathologic examination, providing the gold standard of pathologic diagnosis for gastric cancer diagnosis. Therefore, gastroscopy plays a crucial role in the diagnosis and treatment of all stages of gastric cancer. (Written by Yu Miao, Department of Gastrointestinal Oncology, The First Affiliated Hospital of China Medical University)