Kidney cancer is divided into 4 stages according to the degree of tumor progression, including stages I and II, also known as “limited kidney cancer”, stage III, also known as “locally progressive kidney cancer”, and stage IV, also known as “metastatic kidney cancer”. stage IV is also called “metastatic kidney cancer”. The earlier the stage, the higher the survival rate:
- Stage I: Tumor ≤7 cm, confined to the kidney.
- Stage II tumor >7 cm, confined to the kidney.
- Stage III: Tumor invades peripheral tissues but does not metastasize.
- Stage IV: Tumor metastasized to other organs.
Defining the stage is very important for choosing the appropriate treatment plan. Here is a look at how different stages of kidney cancer should be treated.
Limited kidney cancer (stage I and II)
Surgery is the treatment of choice for limited kidney cancer. There are two types of approaches: radical nephrectomy and unit-preserving surgery (also called partial nephrectomy). The former is recognized by the industry as a possible cure for kidney cancer.
Radical nephrectomy
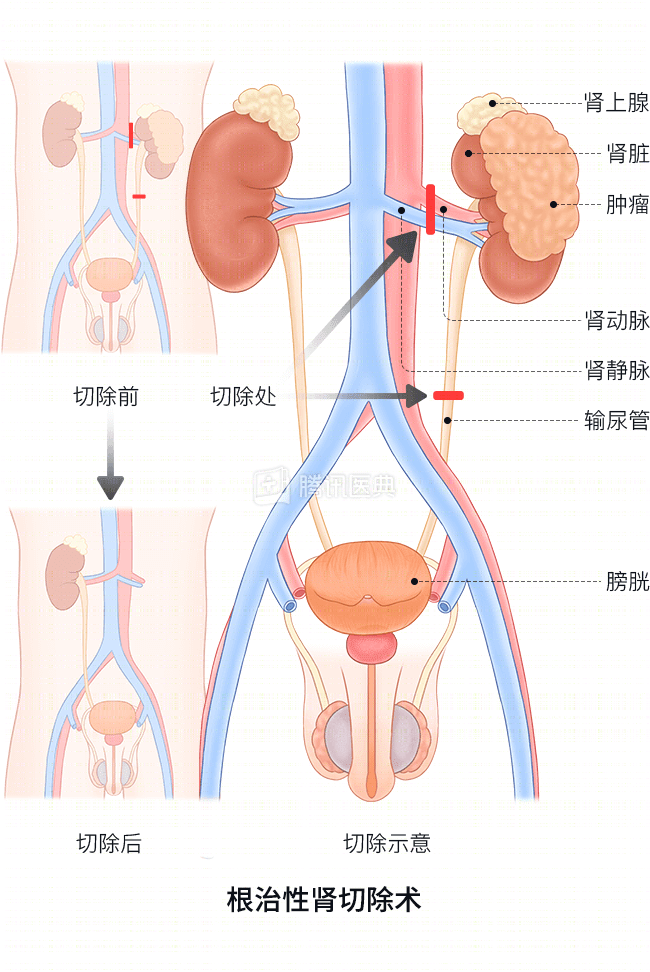
- Population: It is the treatment of choice for those with stage I, but not suitable for partial nephrectomy, and for stage II patients.
- Surgery: It can be done either open or laparoscopically, and both have comparable results. Renal artery embolization is usually not required, and the adrenal gland is usually not removed if the tumor does not directly invade it.
- Risks of surgery: The mortality rate is about 2% and the local recurrence rate is 1% to 2%.
Kidney unit preservation surgery

- Population: In stage I patients, especially those with tumors ≤4 cm, preservation of the renal unit may be considered first. In addition, renal unit-preserving surgery should also be chosen for patients with isolated kidneys (only one kidney), or total renal excision that may lead to renal insufficiency or uremia.
- Surgical Approach: Open surgery is the current standard procedure, but can also be performed laparoscopically.
- Risks of surgery: mortality rate of 1% to 2%, local recurrence rate of 0% to 10%, and postoperative local recurrence rate of 0% to 3% for tumors ≤4 cm.
Other treatments
For patients with small tumors and who are not candidates for surgery, physicians may choose, after evaluation:
- Radiofrequency ablation
- Cryoablation
- high intensity focused ultrasound (HIFU)
But these methods do not allow access to tumor tissue, so a tumor aspiration biopsy is performed before treatment to clarify the pathological diagnosis.
Locally progressive renal cancer (stage III)
In this stage of kidney cancer, the treatment of choice is also radical nephrectomy. However, there is no standard protocol for postoperative adjuvant therapy in the specialty.
Since the tumor has developed lymph node metastases or angiomatous emboli, the physician will choose the treatment on a case-by-case basis.
Metastatic kidney cancer (stage IV)
There is no uniform standard of care for metastatic kidney cancer in the specialty. Surgery is no longer the first choice, but only as an adjunct, as only a very small number of stage IV patients can achieve longer-term survival with surgery. The clinical use of targeted drugs has significantly improved the survival of patients.
Surgical treatment
- Surgical treatment of renal primary focus: In patients with good physical status and low risk*, tumor reduction surgery (removal of part of the tumor to relieve symptoms, also called palliative surgery) should be preferred to help prolong survival. For patients with renal tumors causing severe hematuria, pain and other symptoms, palliative nephrectomy and renal artery embolization can be chosen to relieve symptoms and improve the quality of survival.
- “Low risk” is defined as not having any of the following risk factors.
- Lactate dehydrogenase> 1.5 times the upper limit of normal
- Hemoglobin below normal
- Blood calcium>10 mg/dL
- Time from diagnosis of kidney cancer to start of treatment<1 year
- Kamofsky score (physical status score) ≤ 80
- Number of metastatic organs ≥2
- “Low risk” is defined as not having any of the following risk factors.
- Metastasis surgery: For patients with isolated metastases after radical nephrectomy, and for patients with renal cancer with isolated metastases but in good physical condition, metastasectomy can be performed. Most metastases from kidney cancer occur in the lung, and the 5-year survival rate after surgery for patients with lung metastases is 21% to 60%.
Pharmacologic therapy
The mainstays include cytokine therapy and molecularly targeted drugs, with the latter being more effective.
- Cytokine therapy
- IL-2 (interleukin-2): High-dose IL-2 is indicated for patients with partially recurrent/metastatic, or unresectable, stage IV clear cell carcinoma.
- IFN-α (interferon-α): Medium and high doses are recommended, and the combination with bevacizumab may improve efficacy.
- Targeted drug therapy
- Sorafenib: Recommended dosage 400 mg bid. increasing the dosage or combining with IFN-α may improve efficacy but increase the incidence of adverse events.
- Sunitinib: The recommended dosage is 50 mg qd in a 4/2 regimen of 4 weeks of treatment with 2 weeks off for 1 cycle.
- Other targeted agents: Everolimus or axitinib may be used as appropriate for patients with advanced kidney cancer who have failed treatment with kinase inhibitors such as sorafenib and sunitinib.
Which patients need chemotherapy?
Chemotherapy should only be used for patients with metastatic non-clear cell carcinoma, or metastatic clear cell carcinoma with significant sarcomatoid changes.
Which patients need radiotherapy?
For patients with bone metastases, localized tumor bed recurrence, or regional or distant lymph node metastases, palliative radiotherapy can achieve pain relief and improve quality of survival.
Extended reading:
What is renal cell carcinoma?
Renal cell carcinoma (RCC) is a malignant tumor originating from the urinary tubular epithelial system of the renal parenchyma, also known as renal adenocarcinoma, or simply renal cancer, which accounts for 80% to 90% of renal malignancies.
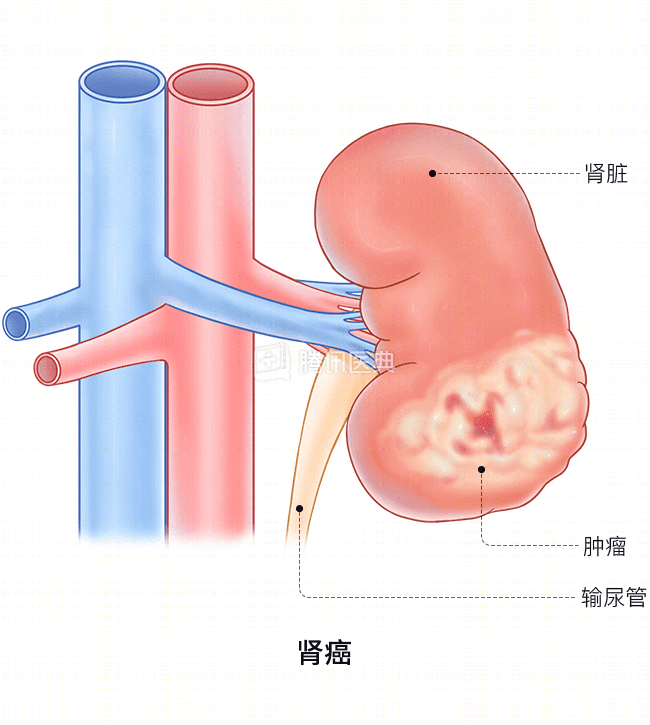
Note: What we commonly refer to as kidney cancer is primarily renal cell carcinoma, excluding renal mesenchymal tumors and renal pelvis cancer.
Is there a high incidence of kidney cancer?
- About 4 to 5 people in 100,000 get kidney cancer.
- More men than women, and more urban than rural.
- It can occur at all ages, with a high incidence at age 50-70.
What causes kidney cancer?
The cause is unknown. The onset is associated with the following factors:
- Heredity: About 2% to 4% of kidney cancers are hereditary.
- Smoking.
- Smoking.
- Smoking.
- Obesity.
- Obesity.
- High blood pressure and antihypertensive treatment.
What types of kidney cancer are included?
The vast majority of patients with kidney cancer in this country have clear cell carcinoma.
The vast majority of kidney cancer patients in this country are clear cell carcinoma, accounting for nearly 90% of cases. Others include:
- Papillary renal cell carcinoma
- Suspected color cell carcinoma
- Collecting duct carcinoma
- Uncategorized renal cell carcinoma
Different types of kidney cancer differ in treatment and patient prognosis.