Common diagnostic methods for gastric cancer include imaging, biochemical and pathological examinations. The pathological examination has the highest accuracy among all the examination methods and is the “gold standard” of diagnosis.
With the development of endoscopic technology, gastroscopic biopsy has become a good means of obtaining pathological samples, and it has been used more often for early screening and diagnosis of gastric cancer because of its advantages of easy sampling, safe operation, and accurate diagnosis. The purpose of gastroscopic biopsy is to study the nature of gastric lesions and to provide a reliable basis for clinical selection of treatment.
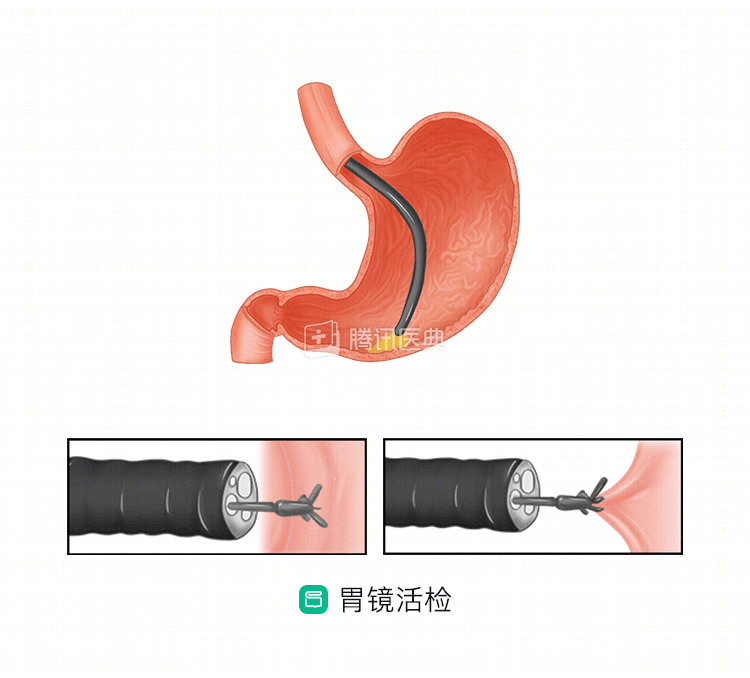
Whether to take a biopsy for gastroscopy depends on the situation
Gastroscopic biopsies are taken primarily from the mucosal layer on the surface of the gastric wall. If the gastroscopy reveals a normal color of the gastric wall, no congestion, erosions or ulcers, smooth mucosa within the stomach, and normal mucosal folds, no biopsy for pathological examination is necessary. For some common chronic superficial gastritis and mild gastric ulcers, biopsy is also generally not needed.
If abnormalities in the mucosa of the gastric wall with severe erosions and ulcers are observed on gastroscopy, the physician will usually take a biopsy to determine whether the lesion is inflammatory or a cancerous ulcer. Many lesions cannot be distinguished by routine gastroscopy, and there is no absolute line between benign and malignant mucosal lesions such as gastric ulcers, which are difficult to distinguish with the naked eye and must be confirmed by taking a biopsy for pathological examination. Pathological examination after gastroscopic biopsy can detect not only cancerous cells, but also cells that are not yet cancerous but have a tendency to become cancerous, such as pre-cancerous mucosal heterogeneous hyperplasia. For suspicious lesions that cannot be characterized, such as changes in mucosal color and luster, changes in mucosal elevation and depression, and interruption of mucosal folds, which cannot exclude the possibility of early cancer, biopsies can be taken with the help of magnifying endoscopy and staining endoscopy.
However, some occupying lesions that originate deep in the stomach wall, such as gastric mesenchymal tumors, gastric smooth muscle tumors, and gastric nerve sheath tumors, cannot be diagnosed by gastroscopic biopsy.
Circumventing contraindications and preventing complications
Biopsy carries the risk of bleeding and perforation. If the patient is taking some antithrombotic medications, such as aspirin, the endoscopist should be informed and the decision to perform a biopsy will be made carefully on a patient-by-patient basis. If a biopsy is needed and the patient is taking medication, the doctor will prepare a hemostatic medication before the biopsy and spray it on the examination site after the biopsy, and the patient will be advised to take oral acid suppressant medication and hemostatic medication, and hospitalization will be recommended for observation if necessary. To prevent the risk of perforation, the doctor will avoid “digging too deep” in the same area.
Gastroscopic biopsy for pathology is a reliable diagnostic tool, and physicians will weigh the need for biopsy in the context of the patient’s specific situation. (Written by Yu Miao, Department of Gastrointestinal Oncology, The First Hospital of China Medical University)