Patients who are suspected of having esophageal cancer should have an upper gastrointestinal barium contrast examination at the time of consultation. This is the most basic imaging method to examine esophageal lesions, which can better show mucosal lesions, tumor length, dynamically observe the movement of the esophageal canal wall, and show the relationship between the esophagus and surrounding tissues.
What is upper gastrointestinal barium angiography?
What is a barium study of the upper gastrointestinal tract?
Commonly known as a “barium meal,” it involves swallowing barium sulfate (contrast agent), which travels through the esophagus to the stomach and duodenum, causing a shadow to develop along the way to diagnose upper gastrointestinal disorders. This is a non-invasive test, and barium sulfate is insoluble in water and lipids and is not absorbed by the gastrointestinal tract, so it is basically harmless to the human body. This test is relatively well tolerated by patients and has few contraindications.
Which patients are not candidates for a barium meal?
.
1. Acute respiratory tract infection;
2. severe cardiac, hepatic, and renal insufficiency;
3. iodine oil or organic iodine as a contrast agent in cases of esophageal or gastrointestinal perforation or esophageal-tracheal fistula or esophageal mediastinal fistula;
4. within 5 days after esophagoscopic biopsy;
5. Acute inflammation of the GI tract, acute bleeding.
What do I need to do before the examination?
1. To ensure that the esophagus and stomach are clean, i.e., free of food debris, you should fast and abstain from water for at least 6 hours before the exam and eat easily digestible food the day before the imaging.
2.
2. 3 days before the exam, abstain from taking high-density medications, such as iodine, bismuth, and iron, which can interfere with the performance of the exam.
How does the procedure work?
.
1. Before imaging, your doctor will have you take 3 grams of gas-producing powder by mouth and swallow 10 mL of warm boiled water to produce about 300 mL of gas to inflate and dilate your stomach.
2. The doctor will prepare the contrast medium, usually about 200 mL of barium sulfate suspension, and have you take a full mouthful (about 40-50 mL) and hold it upright in front of the exam bed.
3. At the beginning of the exam, you will need to assume multiple positions as instructed by your doctor and swallow the “barium meal” in several small bites to ensure that each area of the exam can be well visualized. The general procedure is as follows:
(1) First, perform a chest and abdominal fluoroscopy. Chest fluoroscopy is performed to understand the presence of cardiopulmonary lesions, metastases, etc. The abdominal fluoroscopy is observed for the presence of high-density shadowing that is impervious to x-ray and for contraindications such as intestinal obstruction or perforation.
(2) Right anterior oblique 45° view of the esophagus.
(3) Left anterior oblique 45° to observe again. Double oblique position to observe the passage of barium through the esophagus from different angles and, if necessary, in the prone position to observe esophageal peristalsis.
(4) Lie down, turn 1~2 circles from right to left on the bed (fast speed is required), and then look at the stomach body in the supine position.
(5) In the supine position, look at the body of the stomach and the posterior lateral wall of the gastric sinus in the right anterior oblique position,
(6) In the supine position, the left anterior oblique view of the gastric fundus and the filling of the gastric body, sinus and duodenum.
(7) In the prone position, the anterior wall of the stomach was observed.
(8) In the semiprone position, the right anterior oblique view of the filling of the gastric body and sinus, and peristalsis, etc.
(9) In the semi-recumbent position, the left anterior oblique view of the gastric body and sinus filling, and peristalsis, etc.
(10) In the standing position, drink full barium and observe the filling of the stomach.
(11) In the standing position, observe the compression image.
(12) In the standing position, browse and examine again from the esophagus to the stomach.
How long does it usually take?
Approximately 10 to 20 minutes, or longer if you have poor gastric motility or an obstruction.
What should I expect after the test?
This is a non-invasive test.
This is a non-invasive test and there are no special precautions after the test. You can rinse your mouth with water, spit out the barium residue in your mouth, and then eat and drink normally.
How do the test results look?
The imaging physician will make a preliminary clinical diagnosis based on the imaging presentation of the upper gastrointestinal contrast examination.
1. Typical images of early-stage esophageal cancer (Figure 1) are characterized by disorganized, rough or interrupted esophageal mucosal folds; limited small filling defects (the outline of the barium coating has a limited inward depression due to a small mass in the luminal wall protruding into the lumen, causing the barium to fail to fill); limited stiffness of the canal wall with interrupted peristalsis; small niche shadow, i.e., the site of the broken lesion will be concave A piece, the barium will fill here and develop a shadow, presenting a projection that protrudes beyond the normal contour, just like a niche.
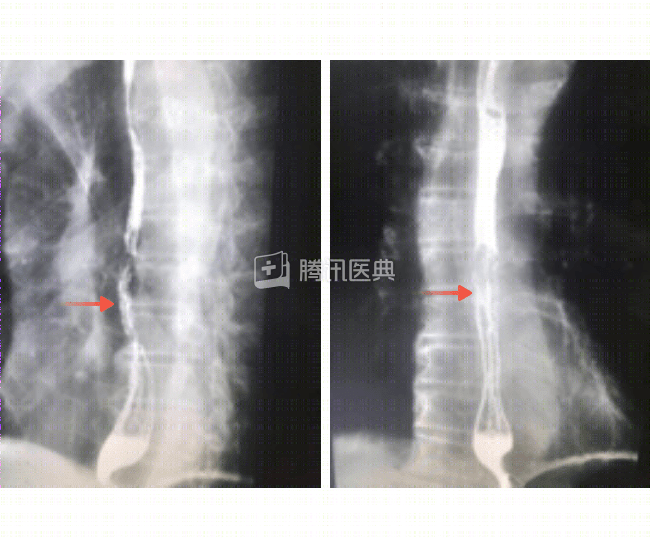
Figure 1: Presentation of early esophageal cancer: left arrow shows disturbed, rough, or interrupted esophageal mucosal folds; right arrow shows small filling defect with limited canal wall stiffness.
2. Images of intermediate and advanced esophageal cancer (Figure 2), often with marked irregular esophageal strictures and filling defects and stiffness of the canal wall. Sometimes, there is varying degrees of dilatation of the esophagus on the oral side above the stricture.
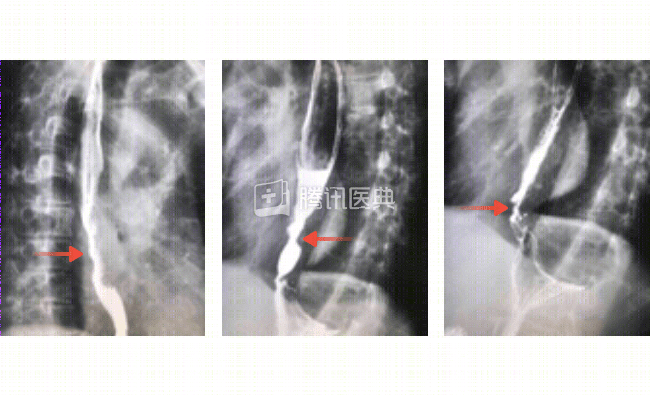
Figure 2: Presentation of mid- to late-stage esophageal cancer: the arrow on the left shows irregular stenosis and filling defect with stiffness of the canal wall; the middle and right images show varying degrees of dilatation of the esophagus on the oral side above the stenosis.
Although the barium meal is noninvasive, it does not visualize images of the lesion and has a relatively high rate of missed diagnoses. Therefore, you need to do further electrogastroscopy on top of that to clarify the diagnosis.