Once kidney cancer is diagnosed, doctors will determine the stage of the tumor, and stage is an important basis for choosing a treatment plan.
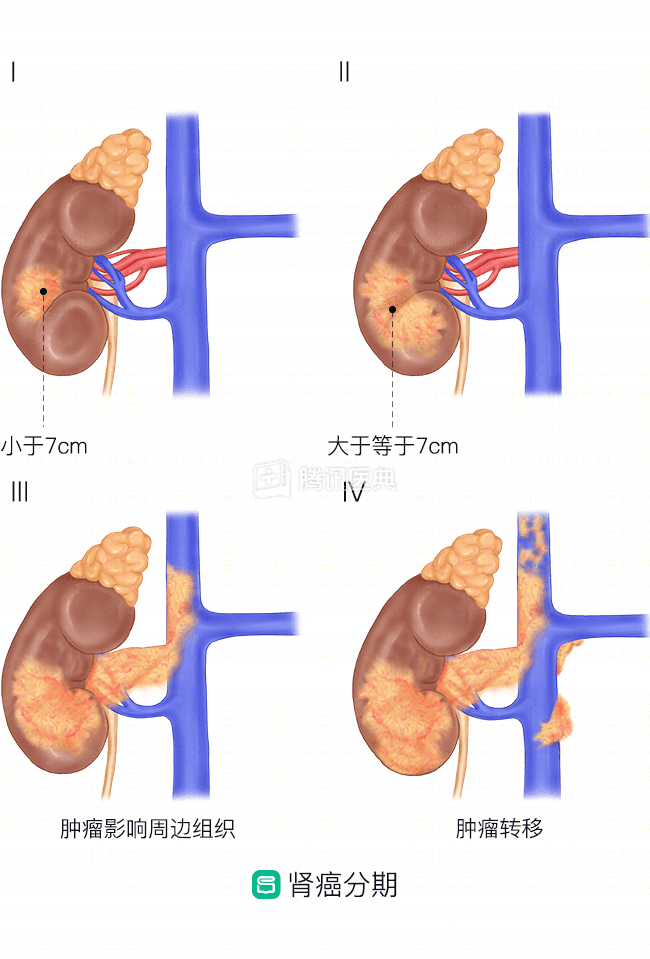
There are four stages of kidney cancer, including stage I and II, which are limited, meaning the tumor is confined to the kidney; stage III, where the tumor has begun to invade surrounding tissues but has not metastasized distantly; and stage IV, which is advanced, where the tumor has metastasized distantly.
The latest National Comprehensive Cancer Network (NCCN) 2019 guidelines pinpoint the treatment options recommended for kidney cancer at different stages.
Stage I
| Table 1. Recommended treatment options for stage I kidney cancer | |
| Stage | Preferred treatment option |
| T1a (tumor ≤4cm in length, confined to kidney) |
|
| T1b (tumor length >4cm but ≤7cm, confined to the kidney) |
|
Stage II and III
Stage II patients have large tumors (>7 cm in length) that are still confined to the kidney; stage III tumors may invade surrounding tissues but have not yet metastasized. For these patients with kidney cancer, the guidelines recommend radical nephrectomy, with partial nephrectomy as an option for those who qualify.
- For patients with clear cell carcinoma (the most common type of kidney cancer) who have a higher risk of tumor progression, the guidelines recommend postoperative enrollment in an adjuvant clinical trial or active monitoring of progression or adjuvant treatment with sunitinib, if available.
- For patients with other types of kidney cancer besides clear cell carcinoma, the guidelines recommend enrollment in a clinical trial after surgery or active monitoring of disease progression.
Stage IV
For patients with stage IV who have developed metastases, based on an assessment of the status of the primary site and metastases, the guidelines recommend the following:
| Preferred Treatment Options | Follow-up treatment | |
| Surgically resectable primary site with oligometastases |
|
If recurrence occurs after surgery, the following treatment options are available:
|
| Surgically resectable primary site with multiple metastases |
|
Same as above |
| Non-surgical resection |
|
Same as above |
|
Table 3. First-line treatment options for recurrent or stage IV renal cancer: clear cell carcinoma |
|||
| Preferred | Second choice | Optional in certain cases | |
| Low risk* patients |
|
|
|
| Medium to high risk* patients |
|
|
|
*Low and intermediate to high risk are defined according to IMDC (International Metastatic Renal Cell Carcinoma Database Consortium) criteria, and the prognostic factors assessed include the following 6:
-
Time from diagnosis of kidney cancer to initiation of systemic therapy <1 year;
-
Poor physical status [assessed by the professional community using the Karnofsky score, with a score of <80% being poor physical fitness];
-
Lower-than-normal hemoglobin;
-
Platelet count higher than normal;
-
Neutrophil counts higher than normal;
-
Corrected blood calcium concentration>10 mg/dL.
Patients were considered low-risk if they did not have any of the above risk factors, intermediate-risk if they had 1 or 2 of the above risk factors, and high-risk if they had 3 to 6 risk factors.
| second choice | Optional in certain cases | |
|
|
|
| Table 5. Systemic treatment options for recurrent or stage IV renal cancer: non-clear cell carcinoma | ||
| second choice | Optional in certain cases | |
|
|
|