
Patients with breast cancer often hear the term “sentinel lymph node biopsy,” but how is this test done? This is described below.
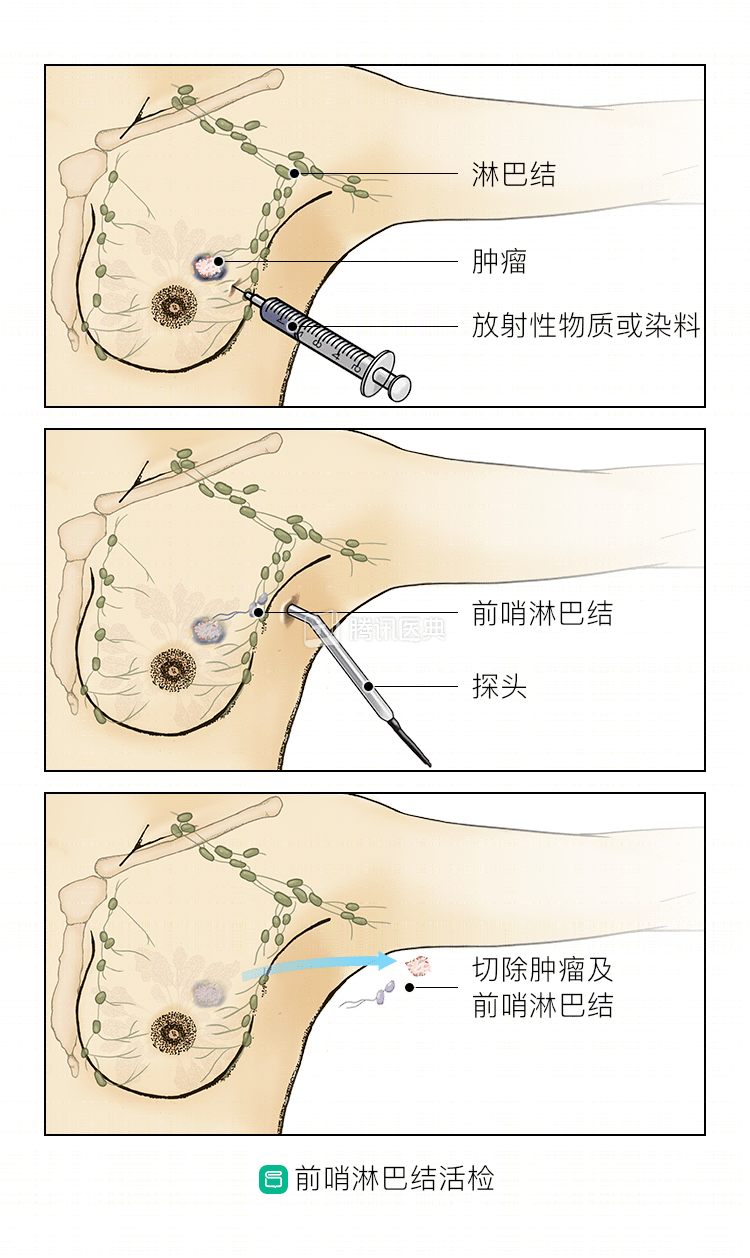
Injection of anterior lymph node tracers
Types of tracers
Tracers for sentinel lymph node biopsy for breast cancer include two major categories: dye tracers, and nucleotide marker tracers.
- The advantage of dye tracers is that they are simple and convenient to perform; the disadvantage is that they have a wide dispersion after injection, and some patients undergoing breast-conserving surgery may palpate hard nodes at the site of dye injection or experience local skin staining.
- The advantage of nuclide tracers is that the “hot spots” of the marked anterior lymph nodes can be detected preoperatively in the axilla with special instruments, and after intraoperative detection and removal of the anterior lymph nodes, the completeness of the removal can be further confirmed based on the nuclear count in the axilla. The radiological safety of the nuclide tracer has been recognized by national and international experts.
Injection site
Regarding the injection site of tracers for sentinel lymph node biopsy, studies have shown similar success rates for both dye and nuclide tracers injected into the tumor surface, peri-tumor intradermal or subcutaneous tissue, and areola area intradermal or subcutaneous tissue.
Time of injection
Whether mastectomy or breast-conserving surgery is performed, anterior lymph node biopsy precedes breast surgery. Nuclear tracers are generally required to be injected 3 to 18 hours before surgery, which can be shortened to 30 minutes before surgery if the intradermal injection method is used, and dye tracers are generally injected 10 to 30 minutes before surgery.
Intraoperative diagnosis of the sentinel lymph node
An accurate, rapid intraoperative diagnosis of the sentinel lymph node allows patients with positive sentinel lymph nodes (ie, with lymph node metastases) to complete axillary lymph node dissection in a single procedure, avoiding a second procedure.
There are two intraoperative diagnostic modalities for sentinel lymph nodes, intraoperative frozen rapid pathology and intraoperative print cytology, either of which can be diagnosed as positive for sentinel lymph nodes and require axillary lymph node dissection.
Postoperative diagnosis of sentinel lymph nodes
Accurate diagnosis of the sentinel lymph node is critical for accurate staging of the axilla, accurate determination of postoperative adjuvant treatment options, and reduction of recurrence rates in the axillary region. A standard postoperative pathologic histologic diagnosis is the gold standard for determining the presence or absence of metastasis in the anterior sentinel lymph nodes. When performing a postoperative pathological diagnosis, the pathologist will section and stain the sentinel lymph nodes, with or without combined immunohistochemical staining. Physicians generally do not consider the routine i.e. application of immunohistochemical techniques to improve the detection of micro-metastases.
After the above steps for axillary sentinel lymph node examination, the physician can perform an accurate analysis of the axillary lymph nodes and proceed to the next step of treatment.