One of the most important concerns of tumor patients is metastasis. Once metastasis occurs in gastric cancer, it will be more difficult to treat, so what are the common ways of metastasis in gastric cancer?
Direct infiltration
Cancer lesions in the stomach can invade directly into surrounding tissues. For example, pancreatic fundic cancer in the “upper” part of the stomach can easily invade the esophagus above the stomach, and sinus cancer near the “exit” of the stomach can easily infiltrate the duodenum below the stomach.
The “spread” of gastric cancer is not just “up” or “down” but may also be “out”. The most important thing is that the patient has a good chance of getting a good understanding of the patient’s condition.

Stomach cancer can also manifest when it metastasizes to surrounding tissues. For example, persistent pain radiating to the lower back can occur when the tumor invades the pancreas. The tumor can infiltrate up to 6 cm beyond the cancer site and up to 3 cm below the pylorus into the duodenum.
Bloodstream metastases
Gastric cancer can also metastasize through the bloodstream, usually in the late stages of gastric cancer, when cancer cells enter the bloodstream and spread to other parts of the body, forming metastases.
The common organs of metastasis for gastric cancer include liver, lung, pancreas, and bone, with liver metastasis being more common. The most common metastases are liver, lung, pancreas, and bone. Bone pain, low back pain, lower limb pain, or shoulder pain may occur in those who develop bone metastases.
Peritoneal implant metastases
Implantation is a very graphic description of how tumor cells can be shed and planted on the surface of the peritoneum and abdominal organs to form metastatic nodes when gastric cancer breaks through the outermost plasma membrane layer.
Usually, the deep fossa in front of the rectum (anterior rectal recess) is prone to form implantation nodes under gravity, and metastatic cancers that occur in the anterior rectal recess can be detected by rectal palpation.
In women with gastric cancer, the tumor can implant into the ovary and form a metastatic ovarian tumor, also known as a Krukenberg tumor. The first manifestation of ovarian metastases from gastric cancer is usually seen in premenopausal or young women, who present with acute abdominal pain, menstrual irregularities, lower abdominal masses, etc., without obvious gastrointestinal symptoms, and both ovaries are often involved at the same time, which can easily be misdiagnosed as simple ovarian tumors.
When widespread peritoneal dissemination of cancer cells occurs, there can be a large amount of cancerous ascites, which can be thin and clear plasma or bloody in nature, and sometimes physicians can use tests to find shed cancer cells from the aspirated ascites.
Lymphatic metastases
Lymphatic metastasis is the main route of metastasis for gastric cancer. The rate of lymphatic metastasis in progressive gastric cancer is as high as about 70%, and early gastric cancer can also have lymphatic metastasis. The rate of lymph node metastasis in gastric cancer is positively correlated with the depth of infiltration of the cancer lesion, that is, the deeper the depth of infiltration, the higher the rate of lymph node metastasis.
There are 16 groups of regional lymph nodes draining the stomach, which can be divided into 3 stations based on their distance from the stomach. The first station is the paragastric lymph nodes, which are organized into groups 1 to 6 in the order of cardia right, cardia left, gastric lesser curvature, gastric greater curvature, suprapyloric, and subpyloric lymph nodes. 7 to 16 groups of lymph nodes are, in principle, in the order of arterial branches: paragastric left artery, paracolic common hepatic artery, paraceliac artery, splenic portal, parapleural artery, intrahepatoduodenal ligament, posterior pancreatic, paracolic superior mesenteric artery, paracolic middle artery, and paracolic abdominal aortic lymph nodes. 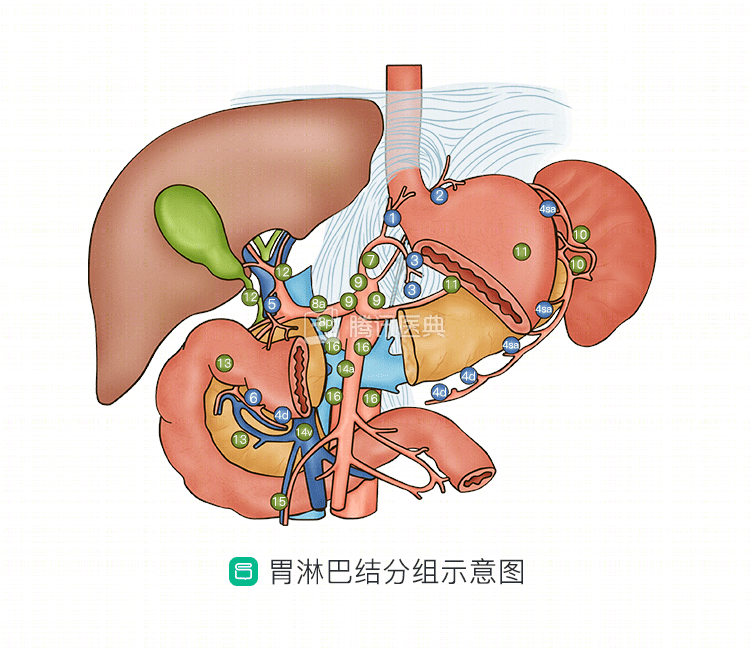
Gastric cancer metastasizes from the primary site to the first station of perigastric lymph nodes via the lymphatic network, followed by centripetal metastasis of cancer cells to the second station along the perivascular lymph nodes that innervate the stomach and may metastasize to the more distant lymph nodes of the third station. The lymph node metastasis of gastric cancer is usually gradual, but jumping metastasis can also occur, i.e. no metastasis in the first station lymph nodes but metastasis may occur in the second station lymph nodes.
Jaundice may occur in the presence of hilar lymph node metastasis from gastric cancer that compresses the common bile duct. In the late stages, gastric cancer may metastasize to the left supraclavicular lymph node via the thoracic duct or to the umbilicus via the hepatic round ligament. During physical examination, doctors may feel enlarged and hard lymph nodes in the left supraclavicular fossa or around the umbilicus. These enlarged lymph nodes may also be detected first and traced to gastric cancer later.
Summary
The most common route of metastasis for gastric cancer is lymphatic metastasis, which can be sequential or jumping to lymph nodes around or distant from the stomach. In addition, gastric cancer may metastasize to important organs such as the liver and ovaries, or infiltrate directly into surrounding tissues. Once gastric cancer is detected, the physician will screen for metastases at the site of potential metastasis as appropriate.