Why can’t a biopsy be done to determine the benignity or malignancy of a tumor if a kidney tumor is present? This is because there are certain problems with a kidney biopsy; it is not like a lump in the breast where a biopsy can determine whether it is benign or malignant, and then the doctor can develop a treatment plan based on that result.
Kidney puncture is not more accurate than CT/MRI diagnosis
A puncture biopsy of a kidney tumor is usually not that accurate – it has the potential to falsely suggest that the tumor is benign, when in fact it is the opposite. And, after all, puncture is an invasive test with some operative risks, such as bleeding and organ damage.
In addition, some benign renal tumors, such as pheochromocytoma, are so similar to renal cancer under the microscope that it is difficult for a pathologist to clarify the nature of the tumor by giving them only such a small portion of the tissue for puncture biopsy, and even a very experienced pathology professor would be unable to do anything about it. Therefore, to make a final determination of benignity or malignancy, it is still necessary to send the whole tumor for pathological examination after the surgeon has removed the tumor completely, and finally the pathologist will make an accurate diagnosis.
So, for most patients, if a CT (computed tomography) scan suggests that the tumor may be malignant, then the patient should be treated surgically according to the criteria for malignancy. Because puncture biopsies are no more accurate than CT or MRI (magnetic resonance imaging), this has led to the still medically unavoidable objective deficiency that at least 10% of all patients with kidney tumors treated surgically end up with pathologic results that show benign tumors.
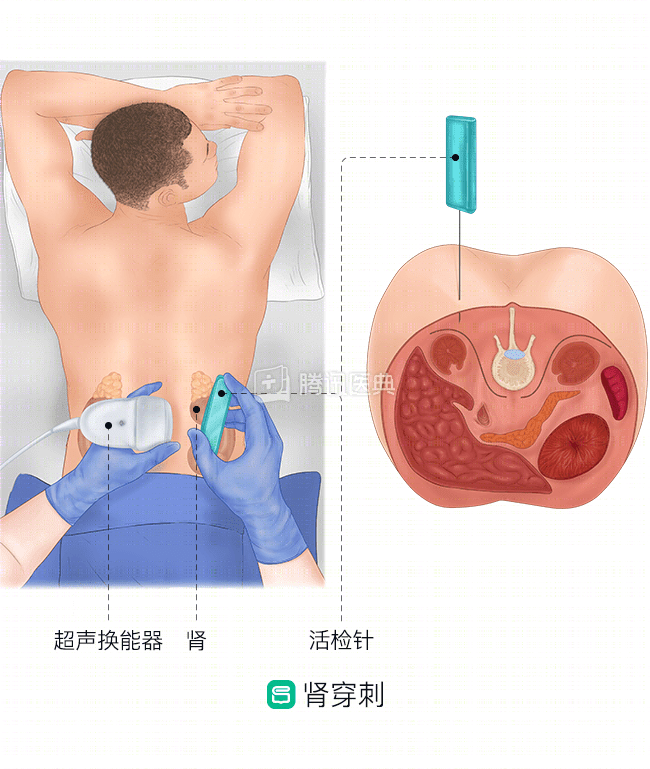
When is a renal puncture indicated?
Puncture biopsy is still relevant in certain specific situations, such as when a patient has a history of other cancers, such as lung cancer or lymphoma, in which case the biopsy can indicate whether the kidney tumor is a metastasis in the kidney from another cancer lesion, and if it is a metastasis, systemic treatment of the other cancer should be an option rather than surgical removal of the affected kidney.
Of course, if the kidney tumor is very advanced and the opportunity to remove the primary tumor is lost (e.g., the patient has a combination of severe cardiopulmonary disease, is in very poor general condition, cannot tolerate surgery, etc.), a puncture biopsy can be used to obtain a pathologic diagnosis, and then targeted systemic systemic therapy can be administered based on this pathologic diagnosis.