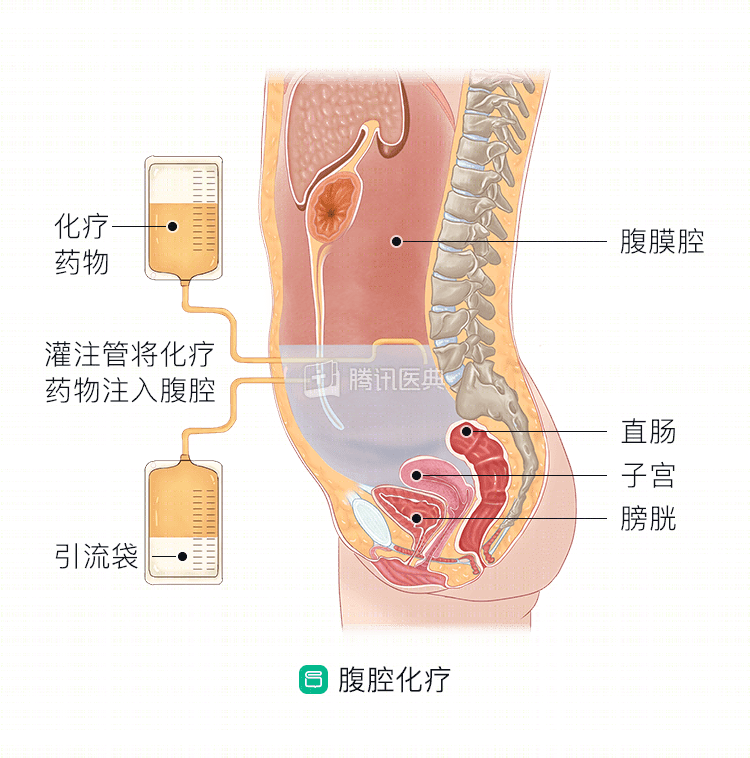
Intraperitoneal chemotherapy, as the name implies, is the injection of chemotherapy drugs into the abdominal cavity. What does this chemotherapy do and in which gastric cancers can it be used? Learn more about it together.
What does intraperitoneal chemotherapy do?
Simply put, the stomach wall is like a “wall” of multilayered structures, with the peritoneum, omentum, and other organs in the abdominal cavity on the outside of the “wall. In the case of deeper infiltration of the stomach wall, it is very likely that some of the cancer cells will penetrate the wall and enter the abdominal cavity, which is one of the reasons why many stomach cancers metastasize peritonally.
The main purpose of injecting chemotherapy drugs into the abdominal cavity is to kill these cancer cells that have penetrated the “wall” to prevent or stop local recurrence and peritoneal metastasis. The main purpose is to kill the cancer cells that have penetrated the “wall” and to prevent local recurrence or metastasis.
In which cases can intraperitoneal chemotherapy be given for gastric cancer?
Patients with gastric cancer may receive intraperitoneal chemotherapy before, during, and after surgery.
- Gastric cancer that has infiltrated deeply enough to penetrate the outermost plasma membrane of the gastric wall, or has developed peritoneal metastases, implant metastases, or malignant ascites, may receive intraperitoneal chemotherapy, potentially converting the tumor to be surgically curable. A Japanese study confirmed the significant efficacy of preoperative intraperitoneal chemotherapy, with an overall efficiency of 56% and disappearance or reduction of malignant ascites in 62% of patients.
- Surgeons may also consider intraperitoneal chemotherapy during surgery to prevent intraperitoneal recurrence and metastasis of gastric cancer if the lesion is found to penetrate the outermost plasma membrane of the gastric wall and is staged to reach cT4a or T4b. Several clinical trials have now demonstrated its positive significance in controlling postoperative recurrence and peritoneal metastasis.
- For the above-mentioned patients with deeper infiltration of gastric cancer lesions found during surgery, or those with positive cancer cells on pathology of abdominal washout fluid, the surgeon may also consider timely prophylactic or therapeutic intraperitoneal chemotherapy postoperatively to prevent intraperitoneal metastasis or recurrence. It is important to emphasize that the physician will pay attention to the “timeliness” of postoperative intraperitoneal chemotherapy. Because the tumor load in the early postoperative period is small, the tumor cells that may remain proliferate faster and are extremely sensitive to chemotherapeutic agents compared to normal tissue, early postoperative intraperitoneal chemotherapy is more effective.
How is intraperitoneal chemotherapy done?
The surgeon will sterilize the skin and administer a local anesthetic to the lower abdomen, then puncture into the abdominal cavity with an indwelling needle. Through an infusion set, fluid heated to a certain temperature and mixed with chemotherapy drugs is injected into the abdominal cavity. After the infusion is complete, compressions are applied.
In the treatment of gastric cancer, the more commonly used intraperitoneal chemotherapy is circulating thermal perfusion chemotherapy (CCCHP), in which the temperature of the circulating perfusion fluid controls the constant temperature of the abdominal cavity to facilitate the penetration of chemotherapy drugs into the tumor cells.
Intraperitoneal chemotherapy is now used in the perioperative treatment of many gastric cancers to help improve patient survival, control local lesions, and improve the quality of survival after treatment.
What are the advantages and disadvantages of intraperitoneal chemotherapy?
Intraperitoneal chemotherapy has the following advantages:
- Lower drug clearance and the ability to maintain high drug concentrations in the peritoneal cavity for long periods of time.
- The drug can enter the liver by absorption, which helps to kill cancer cells that have potentially metastasized to the liver.
- After the drug enters the liver, it is metabolized in the liver into a non-toxic form before entering the systemic bloodstream, which reduces the toxic effects on the whole body, so the drug dose can be increased at the doctor’s discretion.
- Enhanced chemotherapy sensitivity: High temperature can increase the absorption and penetration of drugs into cells, making it easier for chemotherapy drugs to enter cancer cells and kill them, thus enhancing chemotherapy sensitivity.
Intraperitoneal chemotherapy also has certain shortcomings:
- Intraperitoneal instillation can cause local pain and discomfort;
- Chemotherapy drugs entering the abdominal cavity will inevitably cause damage to the peritoneum and other organs;
- May increase the risk of peritonitis, intestinal perforation, fever, anastomotic fistula, and liver and kidney function injury.
Intraperitoneal chemotherapy has been used in the treatment of gastric cancer, but doctors do not have clear definitions on the number of times to use it, the amount of perfusion, and the timing, relying on expert consensus and physician experience, and patients must follow their doctors’ recommendations for individualized treatment. (Contributed by Xin Wang, Department of Gastrointestinal Oncology, The First Hospital of China Medical University)