What is neoadjuvant therapy?
Neoadjuvant therapy is a systemic treatment done before local treatment methods (such as surgery or radiation therapy) are administered to the tumor to shrink the mass and kill invisible metastatic cells early enough to facilitate subsequent surgery, radiation therapy, and other treatments. The most commonly used neoadjuvant treatment in clinical practice is chemotherapy.
For patients with early-stage tumors, they can usually be cured with local treatment options and do not need neoadjuvant therapy, and for patients with advanced tumors, neoadjuvant therapy is usually not used because the opportunity to eradicate the tumor is lost.
For patients receiving neoadjuvant therapy, a new series of imaging tests is needed to reassess whether surgery can be performed. If the surgeon believes that surgery can be performed, it needs to wait until the patient’s blood picture returns to normal, usually some time after neoadjuvant therapy is completed.
Which patients need neoadjuvant therapy?
Prostate cancer growth is highly androgen-dependent, with massive tumor cell death after androgen removal, which for localized tumors manifests as a reduction in tumor size and extent. Therefore neoadjuvant endocrine therapy is often used in the preoperative treatment of high-risk prostate cancer in certain special circumstances.
There are two major categories of “high-risk prostate cancer”
- One category is limited prostate cancer: it has a PSA greater than 20, or a malignancy score of 7 or higher or an International Society of Urologic Pathology ISUP rating of 4 to 5, or a clinically graded T2C tumor.
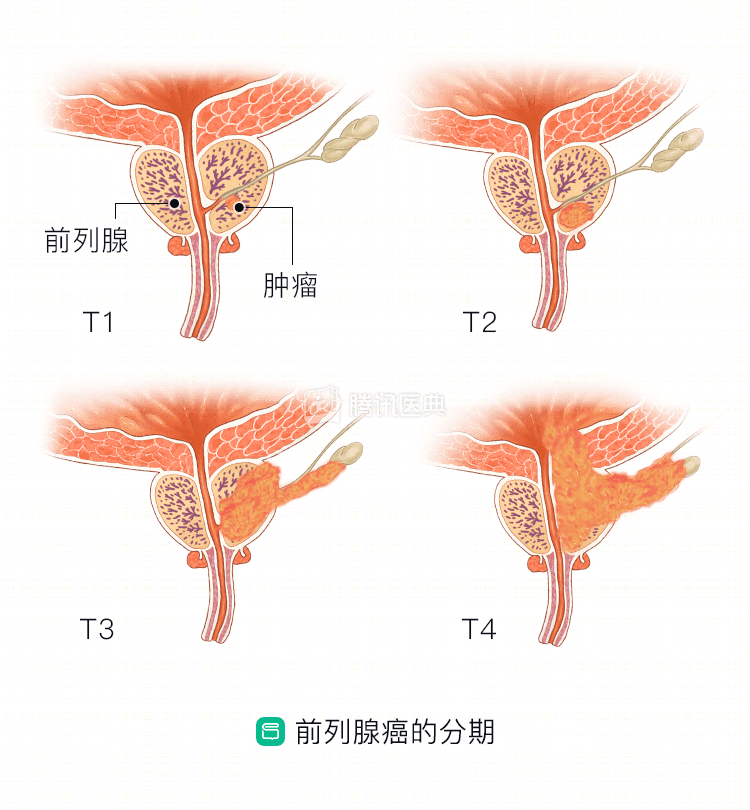
- One category is locally progressive prostate cancer: it is prostate cancer that is clinically staged T3 or T4 or lymph node positive, regardless of its PSA value, GS score, or ISUP rating.
The above-mentioned patients with high-risk prostate cancer do not have good outcomes even though they have undergone surgical resection. The postoperative biochemical recurrence rate (i.e., the incidence of re-elevated PSA) is significantly higher in high-risk patients than in low- and intermediate-risk patients, and the risk of postoperative local recurrence, systemic progression, and death is also significantly higher than in low- and intermediate-risk patients.
For this group of patients, a combination of drug, surgical, and radiotherapy regimens are often implemented to improve prognosis. For patients with high-risk prostate cancer, endocrine therapy is administered for a limited period of time before radical resection to reduce tumor volume, clinical stage, and positive prostate margin tumor rate; then radical reduction surgery is performed to minimize the tumor load in the body; postoperative adjuvant endocrine therapy is taken to reduce local recurrence and distant metastases and improve survival.
In addition, salvage endocrine therapy combined with radiotherapy after biochemical recurrence may also improve long-term survival.
What are the common options for neoadjuvant endocrine therapy?
Neoadjuvant endocrine therapy regimens tend to use a combination of luteinizing hormone-releasing hormone (LHRH-a) and anti-androgens, or LHRH-a or anti-androgens alone, but the combination is more reliable and effective.
The duration of neoadjuvant therapy is typically 3 to 9 months.