Peritoneal metastasis is one of the most common forms of metastasis from gastric cancer and is a major contributor to patient death, with approximately 50% of postoperative recurrences being peritoneal metastases. When the tumor invades the gastric plasma membrane, even if the surgeon performs an extended resection and the surgery is perfect, there is still a great possibility of peritoneal metastasis. This is an important tool to determine whether potential peritoneal metastases are present or even to help remove cancer cells from the peritoneal cavity.
Why laparotomy?
Free peritoneal cancer cells are of critical importance in predicting peritoneal metastases and patient survival. Preoperative cytology by peritoneal lavage is an important way to determine the presence of free peritoneal cancer cells.
In addition to determining the presence of free cancer cells in the peritoneal cavity, postoperative lavage of the peritoneal cavity can help reduce the number of cancer cells that may be free in the peritoneal cavity, which in combination with other means will help prevent the development of peritoneal implant metastases. It has been shown that postoperative localized small amounts of multiple irrigation followed by overall large amounts of irrigation combined with postural adjustment can reduce the residual of exfoliated tumor cells and prevent abdominal and pelvic implant metastasis.
Which patients need abdominal lavage?
Peritoneal lavage is used primarily in patients with gastric cancer staged T3 and T4 and in patients with poorly differentiated adenocarcinoma, during radical gastric cancer surgery.
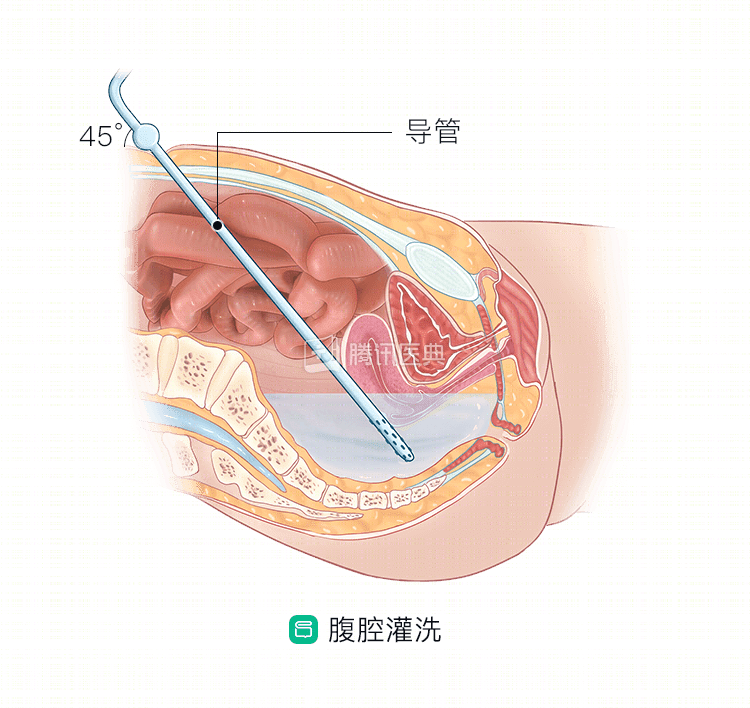
How is laparotomy done?
Traditional lavage of the abdominal cavity is performed during open surgery. The surgeon instills about 500 ml of 37°C saline into the peritoneal cavity before starting radical gastric cancer surgery, and after slow agitation, aspirates it. The irrigation is usually repeated 3 to 6 times. Before closing the abdomen after surgery, the abdominal cavity is flushed with 2000 ml of saline, and the lavage fluid is collected and usually divided into 4 portions to be tested by different methods.
In recent years, with advances in laparoscopic techniques, lavage can also be performed laparoscopically, essentially in the same way as above.
What are the risks of laparotomy?
Some patients may have concerns about whether cancer cells will spread in the peritoneal cavity with the lavage solution. The answer is no. It has been found that when the intraoperative irrigation volume is not less than 3000 ml, tumor shedding cells can be effectively removed, which has implications for the prevention of postoperative abdominal metastasis. In the case of stage II or above gastric cancer, intraoperative lavage after resection of the tumor has a definite effect on the prevention of abdominal metastasis of free cancer cells, and it is easy and safe to operate, with low medical costs and few adverse effects.
In summary, increasing the volume and frequency of lavage not only promotes the clearance of free cancer cells, but also increases the positive detection rate of exfoliated cells, providing a reference for clinical staging, postoperative treatment, and prognosis of patients. (Coauthored by Jianhua Wu, Department of Gastrointestinal Oncology, The First Hospital of China Medical University)