Tumors can wreak havoc on the body’s energy expenditure and the physiology of the digestive tract, often causing malnutrition and immune deficiency, increasing the risk of postoperative complications and infections. If you have poor nutritional levels preoperatively, this may increase the risk of infection and may also affect long-term survival.
Authoritative clinical guidelines all recommend that a preoperative nutritional assessment be performed to objectively evaluate your nutritional risk using a standardized international assessment scale to determine whether you need preoperative nutritional support.
The commonly used dimensions of nutritional evaluation include four areas:
- Routine physical examination: weight, body mass index (BMI), weight change in the last 3 months, waist circumference, upper arm circumference (circumferential length of the midpoint of the upper arm), and also assessment of visceral fat percentage by CT;
-
Blood tests/biochemistry: liver and kidney function, cholesterol/fatty acids, glucose, electrolytes, vitamin/trace element profile;
- Nutrition-related signs and symptoms: appetite, assessment of muscle and subcutaneous fat mass, oral hygiene, hair, skin, nail bed condition, limb edema, oropharyngeal swallowing function (assessed by barium fluoroscopy) and cough reflex function;
- Recent eating status: cooking and eating habits, total daily oral intake, food composition, food allergies and intolerances, effect of combined oral medications on eating status;
.
If your physician assesses that you need nutritional support therapy, you will first have the hospital’s nutritional therapy team (including thoracic surgeons, dietitians, and specialized nurses) educate you about nutritional therapy, including an analysis of the current nutritional risk issues, the nutritional therapy approach, and the overall and milestones expected to be achieved.
Next, your doctor will provide you with nutritional support, mainly enteral and parenteral nutrition.
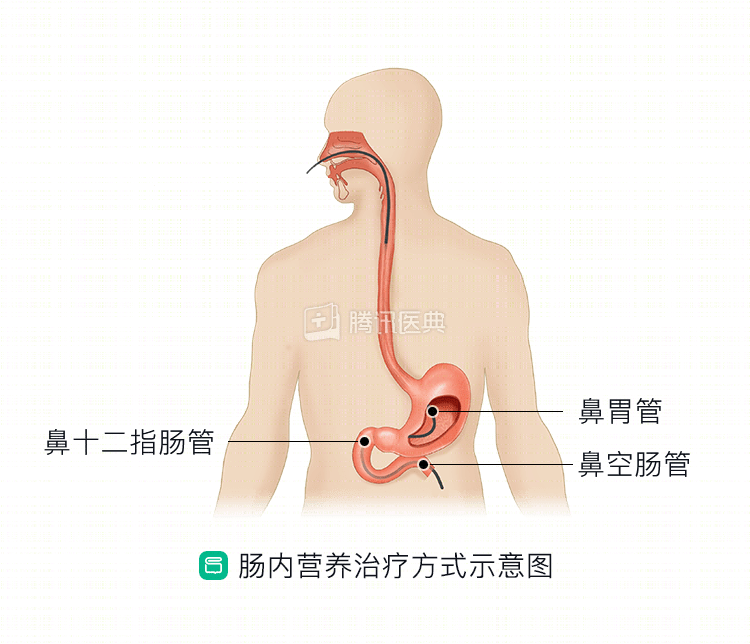
Preferred enteral nutrition support therapy, which relies primarily on indwelling nutrition tubes, can be divided into:
①Tranasal approach (nasal-gastric, nasal-duodenal and nasal-jejunal tubes) (Figure 1);
Transabdominal wall gastrostomy approach;
③Transabdominal wall jejunostomy approach.
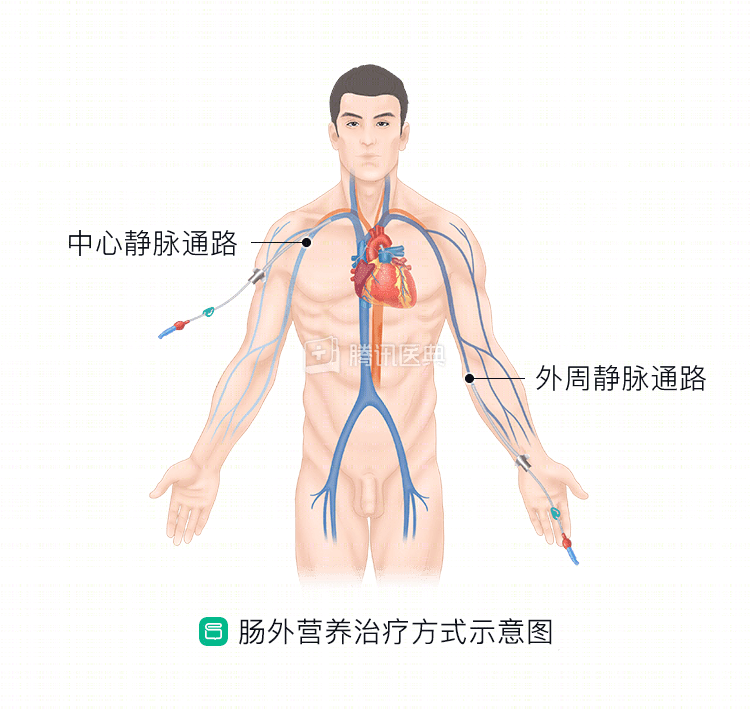
Parenteral nutrition support (nutrition supplied intravenously) is indicated if you have had a complete upper gastrointestinal obstruction prior to treatment (Figure 2).
Nutritional dietary elements include:
Protein, carbohydrate, fat, vitamins, electrolytes, trace elements, and water. Daily therapeutic amounts are calculated based on target caloric intake in kJ.
Medical nutrition solutions will all state the ingredients and total calories on the face of the package.
During inpatient nutrition therapy, changes in nutritional parameters need to be monitored dynamically.
You will also need to stay in close contact with a member of your nutrition therapy team if you need home nutrition support after discharge.
To learn more about preoperative nutrition support, please read: