Both leukemia and lymphoma are among the most common malignancies of the hematologic system, but the clinical presentation and treatment options are different.
First, the origins of the two diseases are different.
Leukemia is a hematopoietic stem cell in the bone marrow that develops malignant clonal proliferation, impaired differentiation, and impaired apoptosis to the point of massive accumulation in the circulation (about 70% of leukemia patients can have leukemia cells in the peripheral blood) and peripheral hematopoietic tissues (liver, spleen) and infiltrates other nonhematopoietic tissues and organs (skin, lymph nodes, nerve centers, etc.) while suppressing normal hematopoietic function and endangering life.
Lymphoma is a malignant tumor originating from lymphatic organs (lymph nodes, liver, spleen, etc.), mostly with a mass as the primary manifestation, invading and metastasizing to various tissues and organs throughout the body and even to the bone marrow (called: lymphoma leukemia stage, which is the end stage of lymphoma), with involvement manifesting as compression and abnormal function of the corresponding tissues and organs, etc.
Second, there are some differences in the predisposing factors and clinical manifestations of the two.
Leukemia is mostly caused by chromosomal mutations due to biological (viral infection), chemical (benzene, chemotherapeutic drugs, etc.) or physical (radiation) factors, etc., resulting in damage to hematopoietic stem cells in a slow accumulation process that generally has 2 to 5 years. Once the disease develops, it can lead to severe anemia, bleeding and infection, enlargement of invaded organs and skeletal pain due to significant suppression of normal hematopoietic function, with a faster progression of disease and more pronounced systemic symptoms.
Lymphoma is most often due to severe infection, stress or disruption of life rhythms that lead to decreased immunity and abnormal clonal proliferation of lymphocytes in the lymphoid tissue. The early clinical stage is often a localized painless mass or relatively slow hepatosplenomegaly. Most patients are seen on physical examination or later in the disease with systemic symptoms such as fever, night sweats, wasting, itching, etc. A small percentage of patients will present with severe anemia and bleeding manifestations.
Furthermore, the two diagnostic methods are different.
The diagnosis of leukemia relies on the results of a bone marrow aspiration smear + biopsy pathology, which confirms the diagnosis based on the morphology, origin, chromosomal mutations, and molecular alterations of the leukemic cells in the bone marrow.
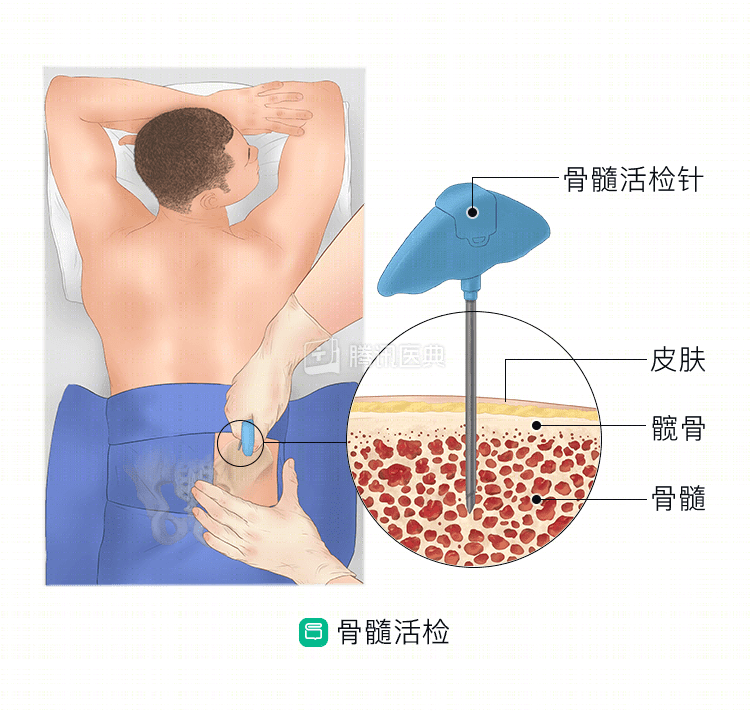
While the diagnosis of lymphoma relies on pathological examination of diseased lymph nodes or tissues and organs, including HE staining and immunoenzymatic labeling, patients with lymphoma also require bone marrow aspiration + biopsy, and that is to determine whether the lymphoma has involved the bone marrow to determine the stage of the disease.
Finally, the principles of treatment and prognosis are different between the two.
Leukemia is mainly divided into myeloid-derived and lymphocyte-derived protoinfantile cell accumulation, and is treated with systemic chemotherapy, which needs to be intense enough to achieve severe bone marrow suppression to kill the leukemic cells, and the course of treatment usually takes about 2 to 3 years, but is highly prone to relapse, and the radical cure is an allogeneic stem cell transplant.
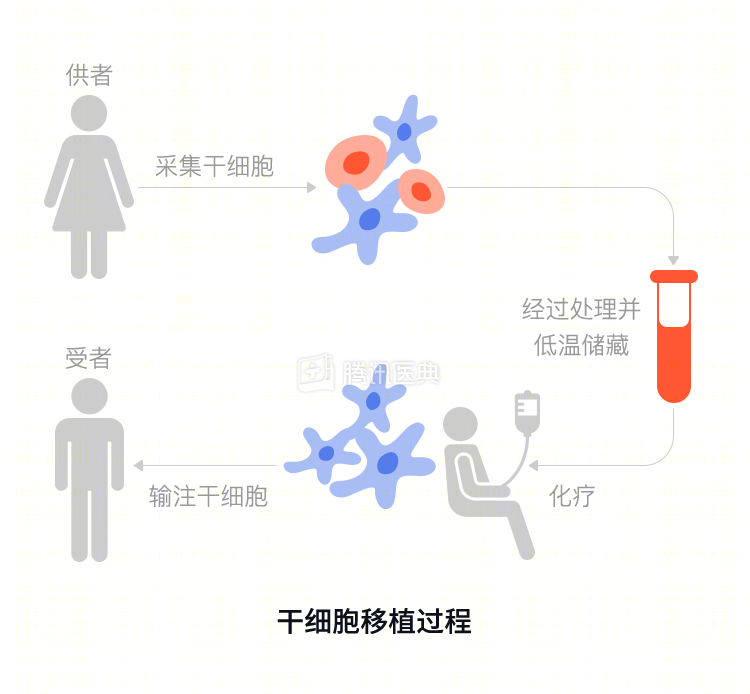
There are nearly 100 pathologic subtypes of lymphoma depending on T and B cell origin, and chemotherapy regimens and prognostic stratification are complex, with a typical chemotherapy regimen of 6 to 8 courses, and the intensity of chemotherapy usually results in only mild to moderate myelosuppression. The patient’s condition is often treated with autologous stem cell transplantation for deeper remission.
Summary
Summary
In conclusion, both types of tumors are malignant diseases that severely affect quality of life and survival, and once they occur, they should be treated in a regular hospital with standardized, individualized stratified therapy for deep remission and long-term survival.