Many patients do not understand the fact that doctors are removing other organs when it is clearly stomach cancer. This is medically known as a combined organ resection, which means that the surgical resection of gastric cancer is not limited to the stomach, but also removes some organs adjacent to the stomach. This article will explain this treatment.
Why do we need a combined organ resection?
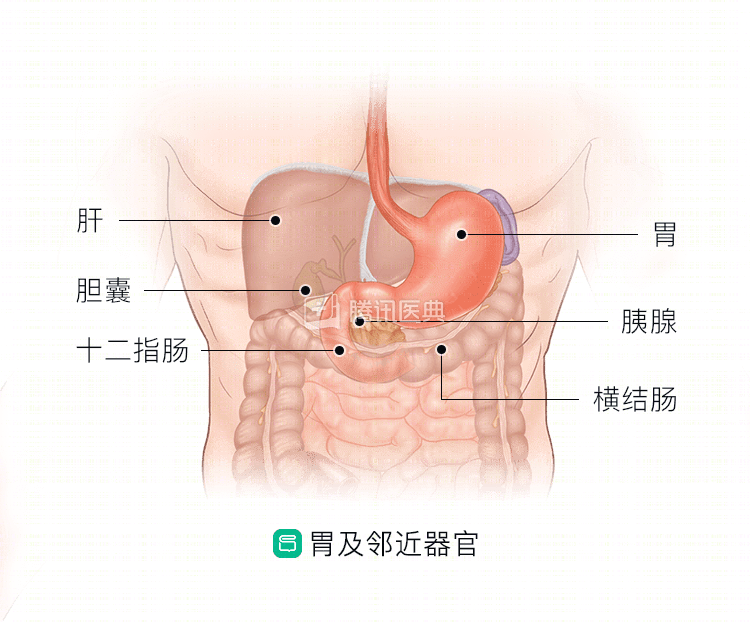
Many patients with gastric cancer are found to be in an advanced stage, and the tumor has invaded adjacent organs around the stomach, such as the pancreas, spleen, transverse colon, gallbladder, etc. There are likely to be lymph node metastases around the stomach as well. Combined organ resection is a treatment strategy aimed at radical cure.
For progressive gastric cancer that directly invades peripheral organs, if distant metastases to other organs are ruled out and the tumor does not invade vital tissues and organs (e.g., vital large blood vessels, adjacent vital organs), physicians will consider combined organ resection if it is safe for the patient and if the patient is physically able to do so.
The combination of combined organ resection with preoperative neoadjuvant therapy and postoperative adjuvant therapy increases the patient’s chances of achieving radical treatment and may provide a survival benefit.
What is the impact of combined visceral resection?
Joint organ resection is more traumatic, patients have a slower recovery, and there may be complications with organs other than the gastric cancer surgery itself.
- Union splenectomy: It is usually used for patients with metastases in the splenic artery lymph nodes and splenic hilar lymph nodes. After combined splenectomy, patients will have a transient increase in platelets, when they are highly susceptible to thrombosis, and thrombosis that occurs in the heart and brain vessels may even be life-threatening. Doctors usually recommend regular postoperative platelet checks, oral antiplatelet medications, and generally a period of antiplatelet therapy for patients after discharge from the hospital.
- Combined partial hepatectomy: The liver is prone to traumatic bleeding after hepatectomy, and liver function may be affected. If preoperative liver function is normal, the remaining liver tissue can often compensate and the liver can usually gradually return to its original size.
- Union cholecystectomy: After removal of the gallbladder, patients may experience symptoms such as diarrhea, avoiding indigestible foods and usually advised to eat less oily foods.
- Joint partial transverse colectomy: It will affect the absorption of water in the intestine, the most important manifestation is diarrhea, and there may also be weakness, oliguria and dehydration, and convulsions. With the addition of an anastomosis to the intestine, there is also an increased risk of postoperative anastomotic fistula, and patients are also prone to diarrhea and other symptoms.
- Union pancreatic tail resection: the main complication is pancreatic fistula in the pancreatic stump, which may cause abdominal infection, bleeding, and abscesses. It may also lead to pancreatic hypofunction, especially since the islet cells are mainly located in the tail of the pancreas, and combined pancreatic tail resection is likely to affect the patient’s glycemic control.
- Union pancreaticoduodenectomy: In addition to complications similar to those of tail pancreatic resection, there may be delayed gastric emptying and slow peristalsis, leading to abdominal distention and belching (hiccups), in addition to postoperative hyperthermia, abdominal pain and distention, jaundice, and peritoneal irritation (i.e., pain and abdominal muscle tension when the abdomen is both pressed and lifted by hand) due to biliary fistula.
In conclusion, combined organ resection is good for “cleaning up” gastric cancer, but it also comes with an increased risk of complications. The physician will choose carefully based on the patient’s condition to maximize the benefit to the patient. (Contributed by Chao Han, Department of Gastrointestinal Oncology, First Affiliated Hospital of China Medical University)