Some stomach cancers that are found early can be cured surgically, and the promising cure for these stomach cancers is radical gastric cancer surgery.
Gastric cancer surgery is divided into radical surgery and palliative surgery. Radical surgery is the primary treatment and the only way to cure gastric cancer. Radical surgery for gastric cancer is surgery in which the primary tumor is removed along with the regional lymph nodes and infiltrated tissue, leaving no tumor remaining and thus potentially curing the gastric cancer.
What are the options for radical surgery for gastric cancer?
Radical surgery for gastric cancer includes endoscopic mucosa resection (EMR), endoscopic submucosa dissection (ESD), and D1 resection for early gastric cancer, and D2 resection for some progressive gastric cancers and enlarged surgery (D2+).
Radical surgery requires complete resection of the primary lesion and complete clearance of the regional lymph nodes. The margin should be at least 3 cm from the lesion for confined growth and more than 5 cm for invasive growth.
The D mentioned above represents the extent of lymph node dissection, with D1 surgery referring to lymph node dissection to station 1 and D2 surgery referring to lymph node dissection to station 2.
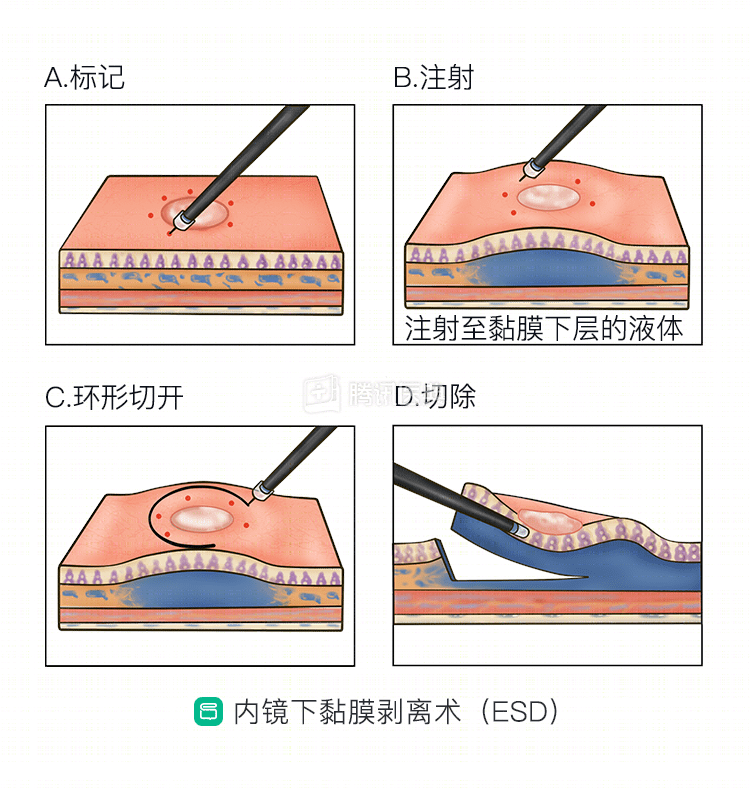
- EMR and ESD are procedures that involve extended resection of the mucosal and submucosal layers with lesions under direct gastroscopic view using a miniature lasso or electric knife, and can be used for highly or moderately differentiated, non-ulcerated, non-lymph node metastatic intramucosal cancers. nbsp;cm is usually treated with ESD, and greater than 3 cm requires surgery.
- D1 resection Intramucosal carcinoma with a diameter of more than 3 cm and gastric cancer that invades the submucosa, doctors usually use D1 resection. Once lymph node metastases are present, a D2 resection is performed.
- D2 resection is the standard procedure for gastric cancer and is usually performed for tumors that have infiltrated deeper than the submucosa (at or beyond the muscularis) or have lymph node metastases but have not invaded adjacent organs.
| Extent of lymph node dissection for D1 and D2 resection of gastric cancer at different sites | |||
|---|---|---|---|
| Distal gastrectomy | Proximal gastrectomy | Total gastrectomy | |
| D1 | 1, 3, 4sb, 4d, 5, 6, 7 | 1, 2, 3, 4sa, 4sb, 7 | 1–7 |
| D2 | D1+8a,9,11p,12a | D1+8a, 9, 10, 11 | D1+8a, 9, 10, 11, 12a |
- Extended surgery (D2+) This type of surgery includes D2 resection + combined organ resection or station 3 lymph node dissection as described above and is indicated for patients whose tumor involves adjacent organs or who present with station 3 lymph node metastases that can be dissected.
Which patients are not candidates for radical surgery?
Some patients with gastric cancer are not eligible for radical surgery.
Some patients with gastric cancer are not candidates for radical surgery, including the following:
- A systemic condition that cannot tolerate surgery;
- Extensive local infiltration that prevents complete resection;
- Conclusive evidence of distant metastases, including distant lymph node metastases, extensive peritoneal dissemination, and more than 3 metastases in the liver;
- Persons with significant defects in vital organ function such as heart, lung, liver, and kidney, severe hypoproteinemia, anemia, and malnutrition that cannot tolerate surgery.
For advanced patients with extensive tumors and metastases that preclude radical surgery, physicians may consider removing only part of the tumor or performing palliative surgery to relieve symptoms in order to reduce pain, maintain nutrition, and prolong life.
Radical surgery is not the whole treatment for gastric cancer
It is important to note that even radical surgery is not the whole treatment, and patients still need to follow medical advice after surgery. Depending on the disease, radiotherapy and some supportive therapy are usually required, and regular follow-up and review should be done to monitor whether the disease recurs and the effectiveness of the treatment.
Postoperative follow-up usually includes blood, imaging, and endoscopy, usually every 3 to 6 months for 3 years after treatment, every 6 months for 3 to 5 years after treatment, and once a year after 5 years of treatment, and endoscopy is recommended once a year.