Hepatocellular carcinoma, known as the “king of cancers,” is one of the most common malignant tumors in China.
The first time the patient was diagnosed with a liver cancer, the patient’s chance for radical treatment such as surgical resection or liver transplantation was lost, and the only option was minimally invasive interventional treatment.
What is large hepatocellular carcinoma? What are the difficulties in its treatment?
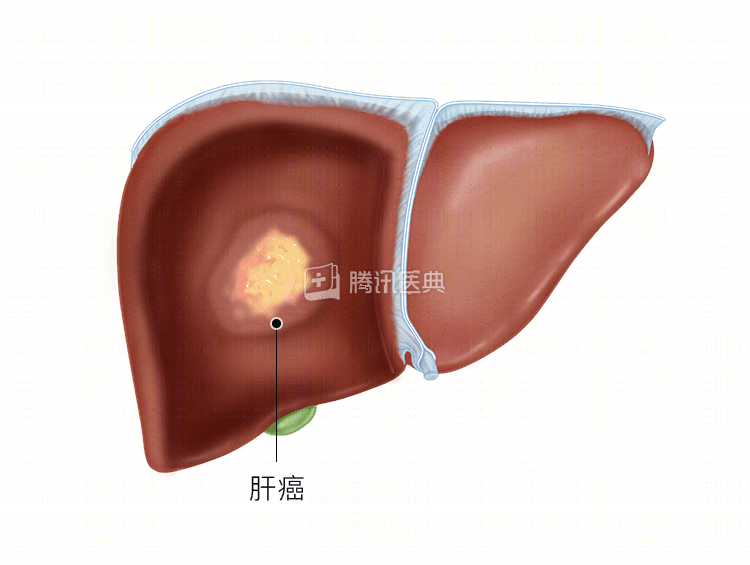
The treatment of liver cancer has long been a challenge for the medical community, especially for large hepatocellular carcinoma, where the results are often unsatisfactory. Large hepatocellular carcinoma is a single hepatocellular carcinoma larger than 5 cm in diameter that grows expansively and has an envelope or pseudo-envelope formation.
Large hepatocellular carcinoma is prone to spread and metastasis, combined with portal vein cancer thrombosis, and compression of bile ducts and blood vessels causing complications such as jaundice, portal hypertension, ascites, and gastrointestinal bleeding.
The same patient with large hepatocellular carcinoma has a highly variable disease that may combine different complications as described above, such as intrahepatic metastases, portal vein cancer embolism, obstructive jaundice, ascites, and gastrointestinal bleeding.
Large hepatocellular carcinoma may be at different stages in the staging of liver cancer, creating great difficulty and complexity in treatment!
Minimally Invasive Interventional Approaches to Large Liver Cancer
The main techniques of minimally invasive interventional therapy include:
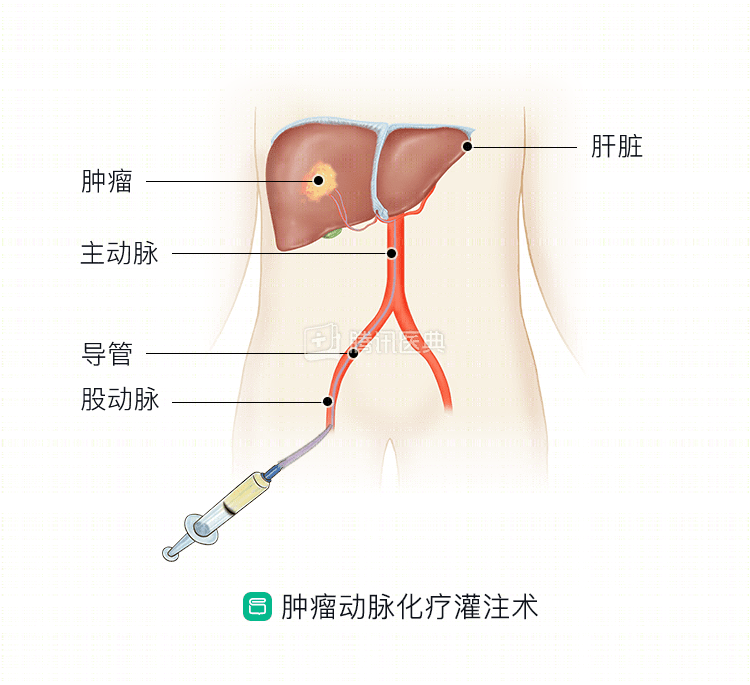
- arterial chemoinfusion (transcatheter arterial infusion, TAI)
- Arterial embolization (transcatheter arterial embolization, TAE)
- Arterial chemoembolization (transcatheter arterial chemoembolization, TACE)
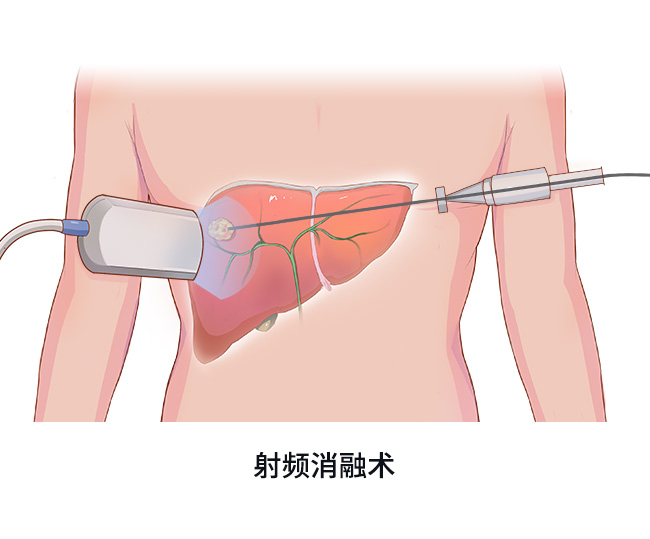
- Radiofrequency ablation
- Microwave ablation
- Radiation particle implantation
The many “weapons” of minimally invasive interventions listed above can be divided into these categories:
- “Irrigation”includes arterial chemotherapeutic perfusion. A catheter is inserted directly into the tumor blood supply vessel to “poison” the tumor by instilling chemotherapy drugs into the tumor blood supply artery. It has high local drug concentrations and low systemic toxicities.
.
- “Plugging”: includes arterial embolization. The catheter is inserted directly into the tumor blood supply vessel, and by injecting embolic substances into the tumor blood supply artery, the tumor blood vessel is blocked, resulting in tumor ischemia and hypoxia, inhibiting tumor growth and promoting tumor cell necrosis and apoptosis. The combination of “irrigation” and “blockage” results in arterial chemoembolization, which is now recognized as one of the most common methods of nonsurgical treatment for liver cancer.
- “Burning” includes radiofrequency ablation, microwave ablation. A two- or three-millimeter diameter needle is inserted into the tumor, and the tip of the needle generates a high temperature of more than 100°C, which directly “burns” the tumor, thus reducing the patient’s suffering from a large incision and avoiding damage to normal organs. The ablation technique is not only used for small hepatocellular carcinomas less than 3 cm in diameter, but also for large hepatocellular carcinomas, which are often combined with TACE to achieve good results.
- “Illumination”: includes radioactive particle implantation. The I radioactive particles are implanted inside the tumor through a fine needle directly into the tumor and are “irradiated” by their radioactivity to destroy the tumor. The company’s main goal is to provide the best possible service to its customers. The technique is mostly used in cases of portal vein cancer embolism, abdominal metastases, lesions that cannot be treated with ablation or TACE, and bone metastases.
Treatment concept of large liver cancer
The heterogeneity of large hepatocellular carcinoma (number of lesions, site of lesions, vascular invasion, extrahepatic metastases, and tumor stage) has guided the selection of treatment options.
Combination therapy is an important part of the comprehensive treatment of large liver cancer, in which different mechanisms and site-specific therapies are combined to achieve a mutually reinforcing and complementary treatment model to compensate for the shortcomings of a single therapy, figuratively speaking, “1+1 is greater than 2”.
The treatment of large hepatocellular carcinoma is primarily a combination of TACE-based interventions.
- For mid- to late-stage large hepatocellular carcinoma, treatment based on TACE shrinks and stabilizes the tumor and interrupts its blood supply source. On the basis of TACE blocking the blood supply to the tumor, combined with ablation (radiofrequency ablation, microwave ablation), the efficacy of TACE is further improved, often leading to the eradication of the tumor.
- For patients with concomitant portal vein cancer thrombosis, the combination of radioactive particle implantation can significantly improve the survival time and prognosis of patients.
In recent years, the emergence of new weapons, “drug-loaded microspheres,” has further improved the outcome of large hepatocellular carcinomas. “The drug-loaded microspheres are embolic substances that can adsorb and carry chemotherapeutic drugs, and enter the tumor blood vessels to embolize them on the one hand, and allow the chemotherapeutic drugs to act inside the tumor for a long time on the other, with the two therapeutic effects overlapping to achieve better treatment.
Summary
In recent years, as basic and clinical research on liver cancer has progressed, the concept of liver cancer treatment has also changed considerably. Given the complexity of large hepatocellular carcinoma and the limitations of various treatment methods, it has become a consensus in the treatment of hepatocellular carcinoma to develop an individualized and comprehensive treatment plan based on tumor characteristics and disease features in combination with different treatment methods.