Difficulty swallowing and gastrointestinal obstruction are among the more common “conditions” encountered by patients with gastric cancer. Why do these problems occur, and how can they be recognized and managed? This article will take a closer look.
Why do you have dysphagia and gastrointestinal obstruction?
Why do you have dysphagia and gastrointestinal obstruction?
Patients with gastric cancer are prone to dysphagia and gastrointestinal obstruction, which are mainly related to the anatomical location and function of the stomach. The upper part of the stomach is connected to the esophagus and the lower part is connected to the duodenum, and the upper and lower parts are called the pylorus.
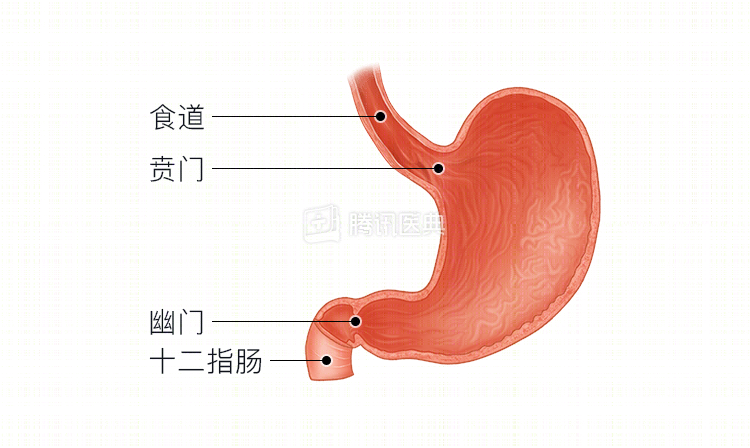
If a tumor blocks the upper or lower “portal” of the stomach, it is likely that food will not pass through the digestive tract, which can lead to difficulty swallowing or gastrointestinal obstruction. If the tumor grows in the cardia, the patient will usually have difficulty swallowing; if it grows in the pylorus, it will easily lead to gastrointestinal obstruction. In addition, if the extent of the gastric cancer lesion is large, the rigid stomach wall itself has poor peristalsis, which can also lead to food retention in the stomach and obstructive symptoms such as abdominal distension, abdominal pain, and vomiting.
What types of obstruction are included?
Any cause that prevents the normal passage of gastrointestinal contents can be called an obstruction. There are many different types of obstruction, and the doctor must first identify which type of obstruction is present in order to provide accurate and effective treatment.
Category by cause
- Mechanical obstruction, the cause of which can be food masses, tumors in the cardia or pylorus, postoperative abdominal adhesions, etc.
- Dynamic obstruction (also called functional obstruction), for example, after gastric cancer surgery, because the nerves around the stomach have been severed or a proximal part of the stomach has been removed, and these nerves or sites that initiate gastric peristalsis are destroyed, which can lead to poor gastric peristalsis.
- Obstructive obstruction of blood flow, due to vascular lesions, stenosis, etc. can lead to poor blood flow to the resected remnant stomach, which can affect gastric motility.
Gastroparesis, one of the common complications after radical gastrectomy for gastric cancer, is a disorder of gastric motility syndrome with impaired gastrointestinal emptying as the main manifestation, and both motility and hemodynamic obstruction etiologies are then usually present.
By obstruction site
- Higher obstruction, such as gastric sinus cancer with pyloric obstruction.
- Low obstruction, e.g., in gastric cancer with pelvic implant metastasis, the implant tumor may cause obstruction with rectal compression.
Accurate determination of the site of obstruction often requires gastroscopy, colonoscopy, gastrointestinal imaging, x-ray, CT, and other tests.
By degree of obstruction
- Total obstruction, as the name implies, means that the contents of the stomach and intestines cannot pass at all. Complete obstruction of the cardia or pylorus of the stomach leads to vomiting after eating, and complete pyloric obstruction also predisposes to vomiting of overnight lodging (food eaten late yesterday or during the night).
- Incomplete obstruction, in which the contents of the stomach and intestines partially pass, results in abdominal distention after eating, which lasts for a long time and slowly and gradually resolves. For example, when incomplete obstruction occurs at the beginning of cardia tumor, patients will choke, have difficulty swallowing or even vomit when eating dry or hard food, but there is no discomfort when eating liquid or semi-liquid food (noodles, congee, chicken cake, tofu brain, etc.), and as the tumor grows into the gastric cavity, difficulty swallowing or even vomiting will gradually occur when eating liquid or semi-liquid food, but there is no obstruction when eating whole liquid food (rice soup, vegetable soup, lotus root powder, etc.), and once complete obstruction The vomiting will occur even when drinking water.
Classification by onset and urgency
- Acute obstruction
- Chronic obstruction
How to recognize obstruction
Gastrointestinal obstruction often presents with abdominal pain, bloating, vomiting, cessation of bowel movements, and persistent abdominal bloating and pain that is not easily relieved after eating, while pyloric obstruction presents with a sour mouth odor or a gastric pattern, in which the upper abdomen bulges in the shape of a stomach after eating, and cardia obstruction presents with choking or vomiting after eating. If these symptoms occur, patients themselves can initially assess their severity to make a preliminary determination of whether obstruction is present and how severe it is.
Any acute, complete, or impaired obstruction requires prompt medical attention. It is important to note that acute gastroenteritis with improper feeding can also result in abdominal distention, abdominal pain, and vomiting, which is self-protective and not entirely obstructive.
How to treat obstruction?
Once an obstruction has been determined, the body is able to treat it.
Once an obstruction is judged, restricting food is the first and most important thing a patient should do. Patients with complete obstruction require strict fasting with no water. In the case of the more common chronic incomplete obstruction, patients can usually take a restricted semi-liquid diet (congee, chicken cake, tofu brain, etc.) or even a total liquid diet (rice soup, juice, milk, soy milk, etc.) to avoid worsening the obstruction. The purpose of restricting the diet is to buy time so that further examination can clarify the classification of the obstruction and choose the appropriate treatment.
For obstruction due to gastric cancer, if the patient is assessed to be able to tolerate surgical radical resection, the surgeon will usually opt for surgery. Surgical treatment not only relieves the obstruction, but more importantly, removes the tumor and may achieve a cure for gastric cancer.
For patients who cannot achieve radical resection with surgery, physicians generally choose palliative resection of the primary gastric cancer tumor, which relieves the obstruction in the short term but often reappears as the tumor progresses.
For patients who are predicted to have difficult surgical resection and poor radicality, physicians may also choose chemotherapy, radiation, and targeted therapy options. These treatment modalities can also shrink the tumor and relieve the symptoms of obstruction. Some hospitals currently carry out endoscopic interventions such as local chemotherapy and particle implantation, which are also local treatments that shrink tumors to achieve relief of obstruction.
For obstruction caused by advanced gastric cancer that cannot be removed surgically or the patient cannot tolerate radical surgery, the surgeon may choose to perform surgical gastrointestinal short-circuiting (also called gastrointestinal anastomosis, similar to rerouting after traffic congestion), gastrostomy (when the cardia is completely obstructed and cannot eat normally, chewed paste-like food can be injected directly into the stomach through gastrostomy), and jejunostomy (similar to gastrostomy, where food is injected directly into the stomach because the stomach cannot utilize it). The first thing you need to do is to have a good idea of what you want to do.
Patients with unresectable tumors with complete pyloric obstruction often require gastrointestinal short-circuiting or jejunal nutrition fistulas, and those with complete cardia obstruction require gastrostomy, while those with incomplete obstruction will attempt to place a catheter or stent, but incomplete obstruction due to cardia tumors is often not suitable for stenting, as stents tend to slip out of place, and continuous stenting is often difficult for patients to tolerate because of esophageal irritation. Percutaneous endoscopic gastrostomy/jejunostomy is more appropriate for patients with gastric cancer that is incompletely obstructed and cannot tolerate surgery. For advanced gastric cancer where the gastrointestinal tract is partially or completely inapplicable, physicians generally choose partial intravenous nutritional support or complete intravenous nutritional support.
Patients with gastric cancer who develop dysphagia or gastrointestinal obstruction should be seen immediately in the hospital, usually requiring fasting and water fasting, and the physician will individualize the patient’s situation after examination and evaluation to determine the cause of the obstruction. (Contributed by Peng Deng, Department of Gastrointestinal Oncology, The First Hospital of China Medical University)