In 1976, experts in blood cell morphology from France (Franch), the United States (American), and the United Kingdom (British) discussed and developed diagnostic criteria for the typing of acute leukemia, referred to as the “FAB” typing.
Since then, the MICM index, which stands for Morphology, Immunology, Cytogenetics, and Molecular biology typing, has been progressively added as a progressive development based on FAB typing. In this case, the cell morphology (M) is the FAB typing.
In 2008, the World Health Organization (WHO) updated the classification of hematopoietic and lymphoid tumors, which significantly improved the diagnostic criteria and prognostic relevance of the WHO classification subtypes.
In 2016, the WHO Classification of Hematopoietic and Lymphoid Tissue Neoplasms was revised and supplemented with the 08 edition, which is the most comprehensive and accurate staging criteria available.
Chemotherapy, targeted agents, and hematopoietic stem cell transplantation are still the mainstay of leukemia treatment. Patients show great heterogeneity in clinical presentation and treatment prognosis, so adequate risk stratification and staging prior to treatment is particularly important for choosing the appropriate treatment pathway.
In acute myeloid leukemia (AML), for example, relevant factors affecting the prognosis of AML patients include:
- White blood cell count;
- Morphologic characteristics;
- immunologic characteristics;
- cytogenetic features and molecular abnormalities, etc.
Among them, cytogenetic and molecular genetic features of AML cells are the most important elements for prognostic determination.
Abnormal karyotypes are found in 50% to 55% of AML patients, and different karyotypic abnormalities predict different prognoses. For example:
- t(15;17), t(8;21), and t(16;16)/inv(16) suggest a desirable prognosis;
- Complex karyotypes, monosomy, t(6; 9), and inv(3) (q21q26) suggest a poor prognosis.
AML can be classified into good prognosis, intermediate prognosis, and poor prognosis groups based on karyotype results, which are significant in predicting disease survival.
The most common mutated genes in AML patients include FLT3, NPM1, DNMT3A, N-RAS, TET2, IDH1/2, CEBPA, RUNX1, TP53, and others. There is a complex relationship between different gene mutations and between gene mutations and karyotype abnormalities, for example:
- NPM1 mutations with negative or low levels of FLT3-ITD suggest a good prognosis;
- NPM1 mutations with negative or low levels of FLT3-ITD suggest a good prognosis;
- FLT3-ITD with NPM1 wild-type, TP53 mutation indicates poor prognosis.
For example, CBFβ-MYH11 gene mutations, corresponding to chromosome inv (16)(p13; q22) and t(16; 16)(p13; q22), such patients are sensitive to chemotherapy and have a better prognosis.
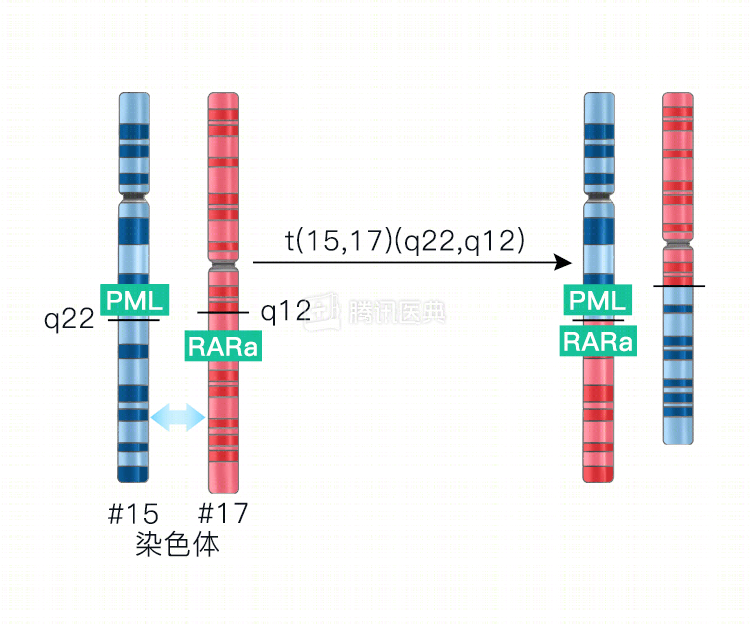
In addition, PML-RARα fusion genes corresponding to t(15; 17) (chromosome 15 and 17 translocation) can be treated with appropriate drugs such as retinoic acid and arsenic, whereas patients with PLZF-RARα or STAT5b-RARα fusion genes are not sensitive to retinoic acid therapy.
This shows that accurate typing of leukemia not only facilitates early and accurate diagnosis of acute leukemia, but also facilitates the selection of treatment options and prognosis. The study of cytogenetic and molecular biology mechanisms in the development of acute leukemia and the use of leukemia-specific targeted drugs in the clinical setting have pushed the treatment of acute leukemia into the “precision therapy” mode.
The movie “I am not a druggist” also relies on precise typing of chromosomes and genes of patients in the early stages of leukemia to select targeted drugs for miraculous results. And for those patients who are already judged to be at high risk at the time of diagnostic typing, a relatively strong induction regimen with sequential bone marrow transplantation can be chosen at the beginning of treatment to achieve the longest possible survival.