Pain is one of the “troubles” that oncology patients face, not only limiting their activities, but also affecting their sleep and causing some negative emotions that can seriously reduce their quality of life.
Stomach cancer pain is generally classified as postoperative pain and pain due to progression of the cancer. Different stages of gastric cancer may lead to different levels of pain, such as vague pain in the early stages, persistent pain in the late stages or after metastasis, and just like other surgeries, patients with gastric cancer can face pain after surgery. In any case, patients should not just “tolerate” pain, but “treat” it.
What are the principles of analgesia?
What are the principles of analgesia?
Patients with gastric cancer should not tolerate pain without medical attention or self-medication, and pain relief should be standardized under the guidance of a medical professional. The World Health Organization (WHO) has proposed a three-step medication principle for cancer pain management, which follows the following principles:
- Emphasis on stepwise dosing from weak to strong and gradually increasing dosage, doctors usually do not wait until the patient feels the need to use the medication, but use it regularly and on time;
- Oral dosing, as the best route, and if oral dosing is not possible rectal or transdermal dosing should be considered, avoiding invasive routes of dosing as much as possible so that patients can take them for a long time;
- Take the medication on time. The physician will emphasize taking the medication regularly and on time rather than on demand (when the pain is felt), thus ensuring continuous pain relief;
- Individualized dosing, where the goal is to achieve effective analgesia without the so-called “extreme” dose.
For postoperative analgesia, it is important to note that postoperative pain relief is not as painless as possible. Analgesic drugs have an impact on postoperative recovery due to side effects such as drug accumulation, which may mask the true condition and result in postoperative irritability, drowsiness, delirium, respiratory depression, and increased heart rate. Therefore, postoperative analgesia will be applied at the doctor’s reasonable discretion.
What are the commonly used analgesic medications?
According to the three-step dosing principle, physicians usually use different medications at different steps of the ladder.
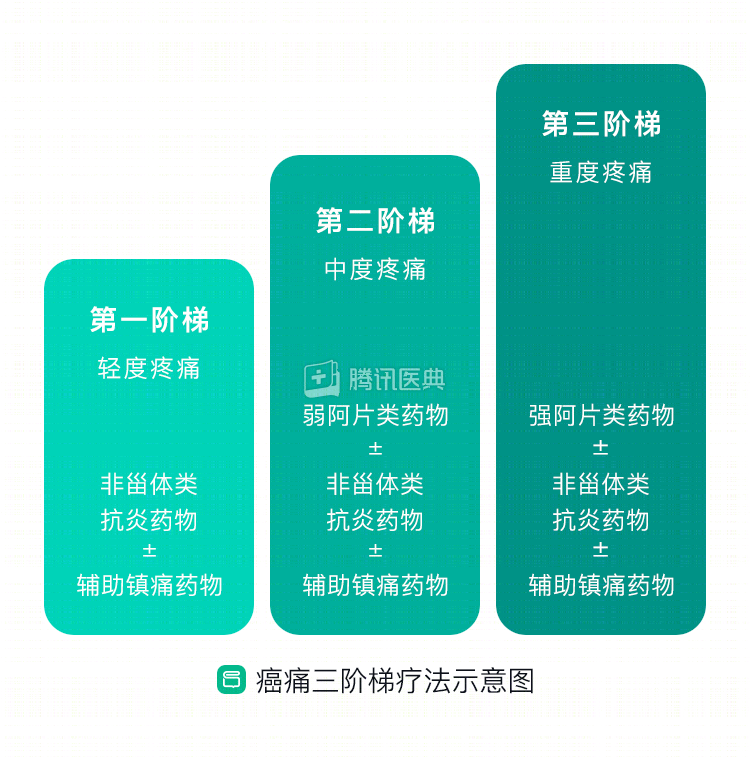
First step
For mild pain, physicians typically give non-opioids (NSAIDs), possibly supplemented with some pain medication. NSAIDs suffer from a maximum effective dose problem, meaning that after a certain dose the pain relief does not increase again even if the dose is increased further. Drugs commonly used on this ladder include acetaminophen (commonly known as paracetamol), aspirin, diclofenac, a combination of acetaminophen and caffeine (plus heparin), ibuprofen, and indomethacin.
Non-steroidal anti-inflammatory drugs are not addictive, and their possible adverse effects are listed below.
- Gastrointestinal reactions. These include epigastric discomfort or vague pain, nausea, vomiting, fullness, belching, loss of appetite, and other dyspeptic symptoms. Peptic ulcers can occur in patients taking oral NSAIDs for long periods of time, and in a very small number of these patients, serious complications such as bleeding or perforation can occur.
- Liver damage. At therapeutic doses, some patients will develop mild liver damage, as evidenced by abnormal blood test markers (biochemical tests), and may develop jaundice, hepatitis, and liver dysfunction.
- Neurological adverse reactions. Patients may experience headache, dizziness, tinnitus, deafness, amblyopia, drowsiness, insomnia, abnormal sensation, and numbness. There are also some less common symptoms such as hyperactivity, excitement, hallucinations, and tremor.
- Urologic adverse reactions. The main manifestation is peripheral edema. Patients may have urinary protein, tubular, red blood cells, white blood cells, and other components that are not normally present or are present in small amounts in the urine.
- Hematologic adverse reactions. Some drugs can cause leukopenia, aplastic anemia, and coagulation disorders.
- Allergy. Some patients may develop allergic reactions such as rash, angioneurotic edema, and asthma.
For these adverse reactions, physicians generally take the following measures to prevent them: rational selection of the variety and dosage form of the NSAID; individualized dosing; safety monitoring; and determining whether the patient has a contraindication to the use of the drug. In the event of an adverse reaction, physicians will generally consider discontinuing the appropriate drug as appropriate and provide symptomatic treatment.
Second order
For moderate pain, physicians usually give weak opioids, possibly along with some NSAIDs and pain medications. Weak opioids also have a maximum effective dose. Commonly used drugs in this order are codeine, brucizine, and tramadol.
Third step
For severe pain, doctors give opioids and may use some NSAIDs and painkillers together. There is no maximum effective dose of strong opioids, but tolerance can develop and appropriate dose increases are needed to overcome tolerance. Many patients refuse to use morphine for pain because they think it is addictive. In fact, morphine is rarely addictive for cancer pain patients. The drugs commonly used in this step are morphine as well as morphine extended-release and controlled-release tablets, and morphine controlled-release tablets can be administered through the rectum.
Opioids are rarely addictive and may cause the following adverse reactions.
- Constipation is most common in long-term opioid users, mainly because opioids depress the central nervous system and make it insensitive to bowel “signals”.
- Nausea and vomiting depend on how the medication is given, how sick you are, etc.
- Itching.
- Itching. Analgesics can trigger the release of histamine, which can cause itchy skin.
- Drowsiness is most common at the start of opioid therapy or with large dose increases.
- Delirium is a common presentation in patients with advanced cancer, and most patients develop delirium in association with opioid use.
- Respiratory depression is the most serious adverse effect of opioids, but is rare.
Caregivers will closely monitor the patient’s condition, watch for changes in vital signs, and take proactive precautions. When using analgesics, physicians usually start with small doses and standardize progressively higher doses. When dose-related adverse reactions occur, the dose is usually reduced. In addition to symptomatic management for adverse reactions, there may be a switch to another opioid or a change in route of administration.
For refractory cancer pain, doctors may also treat it with ultrasound interventions, nerve blocks, and so on. Some patients with gastric cancer are reluctant to interact with others, which can lead to bias in pain assessment and treatment. Patients and family members should actively and honestly cooperate with physicians to achieve the best analgesic effect.