Esophageal cancer is a malignant tumor that occurs in the esophagus and originates from the epithelial cells of the esophagus.
Under constant stimulation by multiple internal and external factors, normal esophageal tissue cells undergo repeated processes of injury, repair, and accumulation of genetic mutations, gradually forming squamous epithelial hyperplasia or columnar epithelial metaplasia.
Squamous epithelial hyperplasia (Figure 1) is an abnormal proliferation of otherwise normal squamous epithelial cells in the esophagus. It is a benign lesion, but requires regular gastroscopic monitoring and vigilance for cancer if moderate to severe atypical hyperplasia is found.
Columnar epithelial metaplasia (Figure 2) is a precancerous lesion in which the squamous epithelium is covered by abnormal columnar epithelium that may further develop into adenocarcinoma.
When these stimuli reach a “tipping point,” the cells can “grow” uncontrollably and become cancerous.
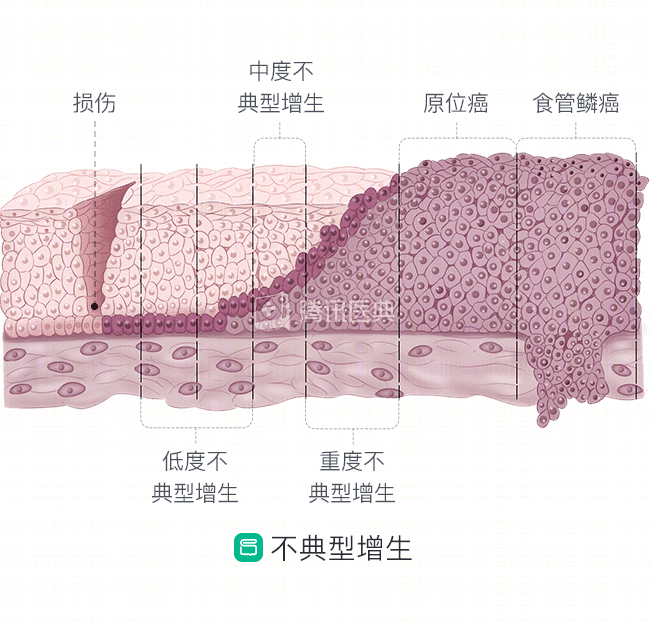
Figure 1
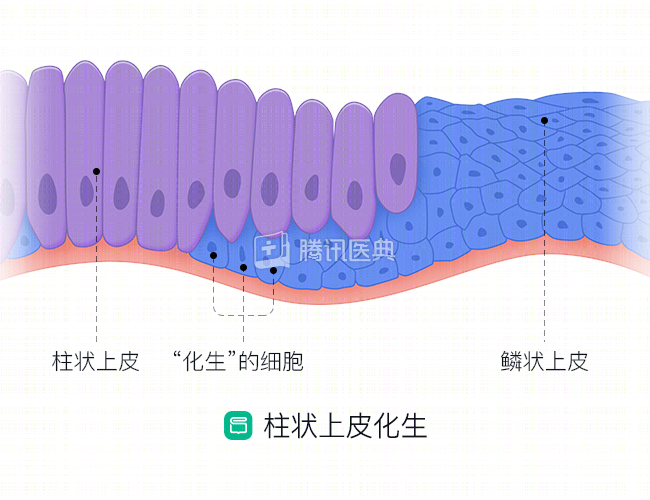
Figure 2
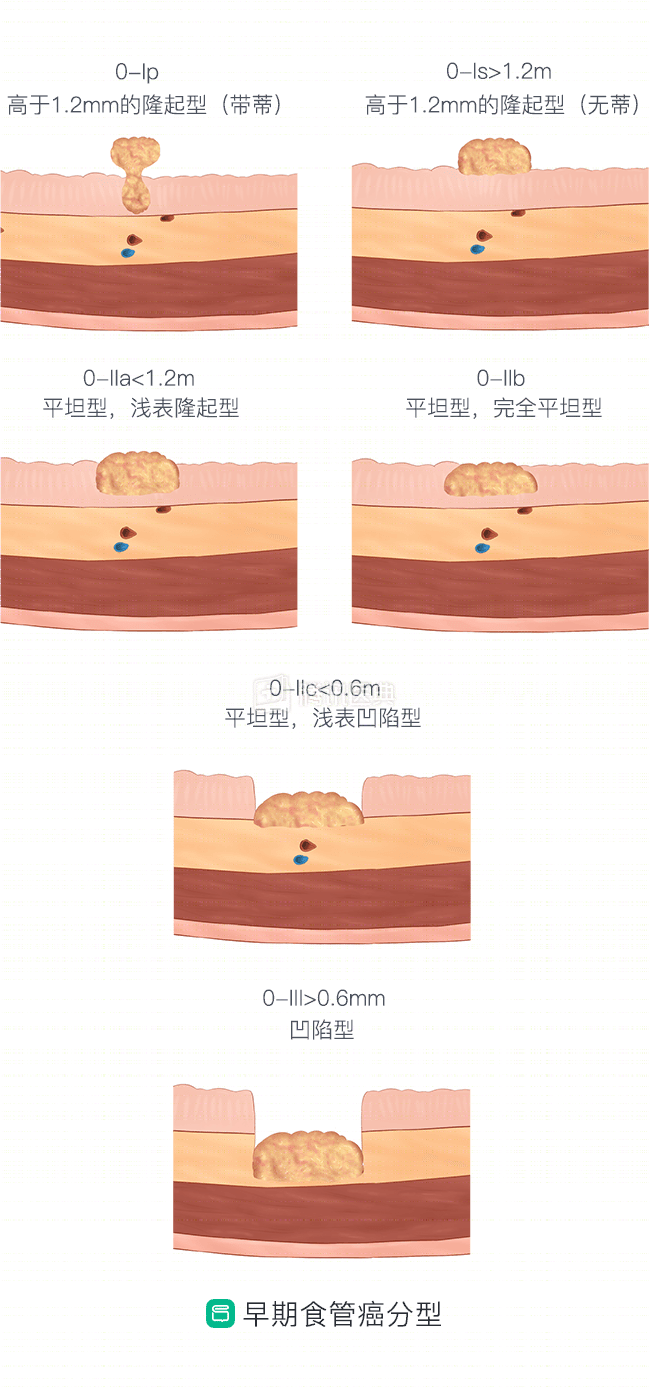
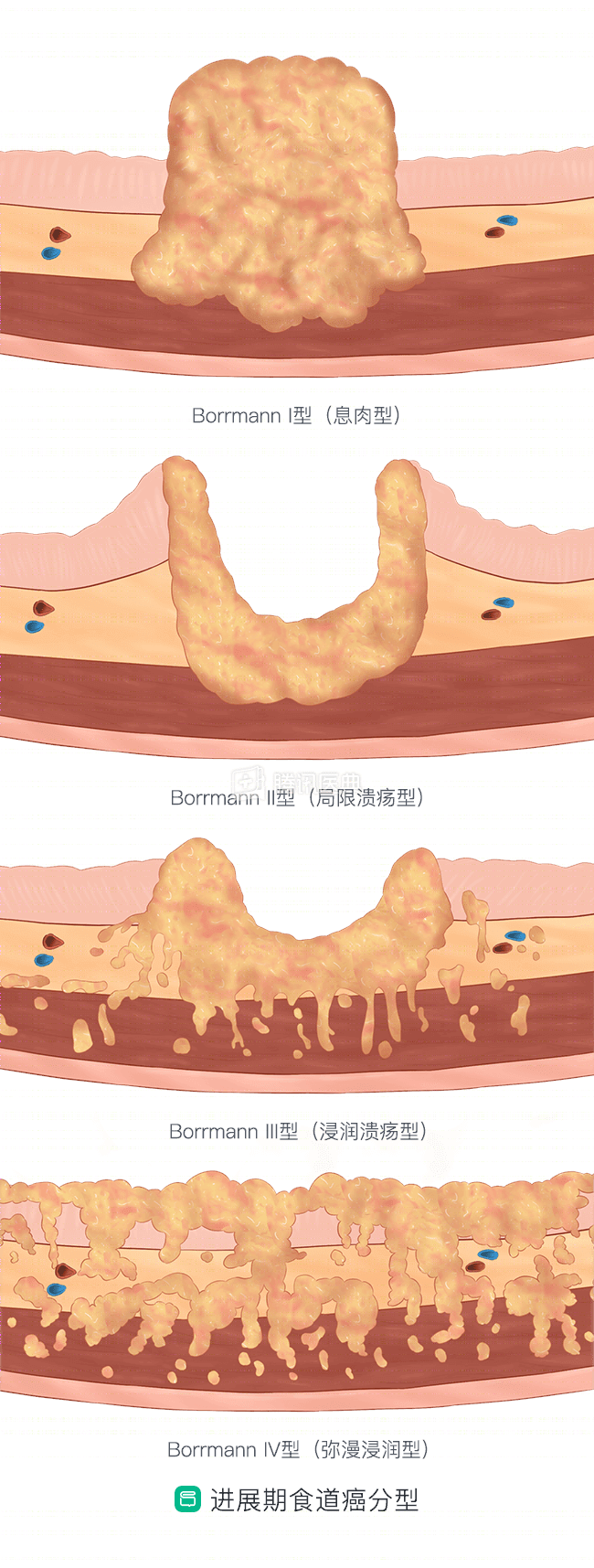
Which types of esophageal cancer are classified
According to the pathological type, esophageal cancer is mainly divided into squamous carcinoma and adenocarcinoma, which can be divided into 4 subtypes: simple adenocarcinoma, adenosquamous carcinoma, mucinous epidermoid carcinoma, and adenoid cystic carcinoma. There are few other pathological types of esophageal cancer, such as basal cell carcinoma, neuroendocrine carcinoma, and esophageal sarcoma, all of which are very rare.
Squamous carcinoma is a tumor that forms in the squamous cells of the esophagus, usually at a physiologic or pathologic stricture that occurs in the middle or upper part of the esophagus. In China, about 90% of esophageal cancers are squamous.
Adenocarcinoma is a malignant tumor that occurs in the submucosa of the esophagus, or from the cardia glands. Adenocarcinoma is the predominant type in Europe and the United States.
To learn more about the difference between squamous carcinoma and adenocarcinoma, please read: