Laparoscopic surgery, a newer minimally invasive surgical procedure, has become more and more familiar in recent years, and is well accepted among patients because of its advantages such as less trauma, less bleeding, faster postoperative recovery, and smaller incisional scars. The first question many gastric cancer patients ask after they are sure they need surgical resection is often, “Can I have laparoscopic surgery?” The following will answer that question.
What conditions are eligible for laparoscopic surgery?
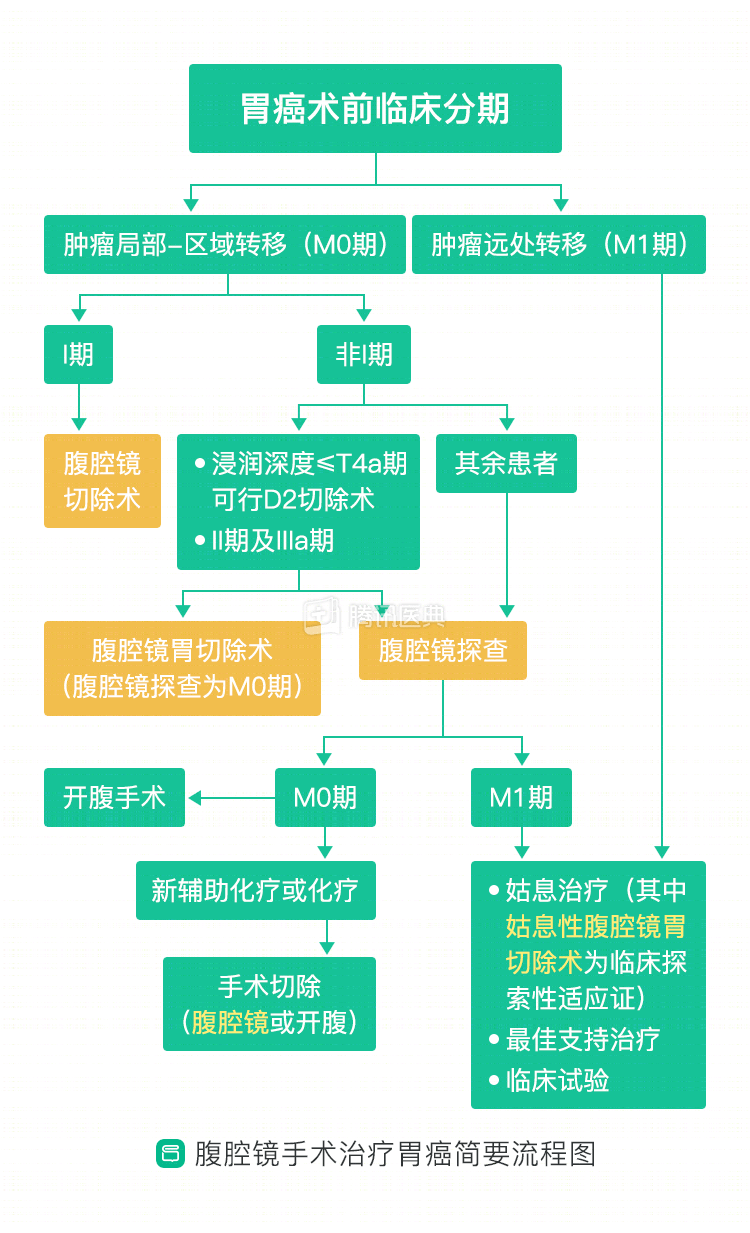
China’s latest Guidelines for the Operation of Laparoscopic Gastric Cancer Surgery state that the following patients with gastric cancer can undergo laparoscopic surgery:
- Gastric cancer exploration and staging.
- Gastric cancer with tumor infiltration no deeper than stage T4a, and D2 radical resection can be achieved (D2 resection is the standard procedure for gastric cancer; D2 is the clearance of lymph nodes to station 2 lymph nodes).
- Preoperative staging of gastric cancer is stages I, II, and IIIa.
- Short-circuit surgery for advanced gastric cancer.
The above indications have been recognized and applied in clinical practice. In addition, there are a number of conditions that are currently being explored in clinical practice with laparoscopic surgery, including:
- Gastric cancer with preoperative assessment of the depth of tumor infiltration at stage T4a and achievable D2 radical resection.
- Palliative gastrectomy for advanced gastric cancer. (See below for a brief flow chart)
What conditions preclude laparoscopic surgery?
Of course, laparoscopic surgery is not a panacea and cannot be performed if the following conditions are evaluated by the surgeon:
- Pneumoperitoneum must be established before laparoscopic surgery to separate the abdominal wall from the organs and expand the abdominal cavity to facilitate the surgery, and laparoscopic surgery cannot be performed if the patient is assessed to be unable to tolerate a pneumoperitoneum or if a pneumoperitoneum cannot be established.
- Patients with extensive intra-abdominal adhesions that are difficult to visualize laparoscopically.
- Age not less than 80 years (advanced age);
- Body mass index (BMI) of not less than 25 kg/m (overweight);
- Exertional expiratory volume in one second (FEV1)/expected value not greater than 50% or FEV1/exertional spirometry (FVC) not greater than 60% (ventilatory dysfunction);
- Heart ejection fraction not greater than 50% (cardiac insufficiency);
- Have a high risk of thrombosis, etc.
In addition, different patients with gastric cancer may be at different risk for laparoscopic surgery depending on their physical status and will be systematically evaluated by the surgeon prior to treatment. Although there is no uniform risk assessment tool, physicians are particularly vigilant and cautious in assessing whether laparoscopic surgery is acceptable in the following situations:
In conclusion, laparoscopy as a minimally invasive surgical modality can be used for some patients with gastric cancer after comprehensive evaluation by the surgeon, but those who have contraindications to laparoscopic surgery or are assessed to be at high risk should still be selected with caution. (Contributed by Han-Yu Chen, Department of Gastrointestinal Oncology, The First Hospital of China Medical University)