Pathology is the examination of human tissue and cells, also known as biopsy and cytopathology, respectively. The pathologic diagnosis is the “gold standard” for tumor diagnosis and provides an important basis for determining the benignity and malignancy of the tumor and its pathologic stage.
The collection of pathological specimens is crucial in pathological examination, and this article explains how to obtain specimens for pathological examination of gastric cancer.
How do physicians obtain tissue specimens?
Intraoperative frozen biopsies are rarely performed for gastric cancer. For patients with suspected gastric cancer, physicians obtain routine biopsy specimens primarily through the following routes.
Therapeutic surgical resection
The therapeutic surgical resection route, in which specimens are obtained by surgical resection for therapeutic purposes, is generally used in patients with undefined preoperative pathology who require intraoperative pathology to determine further surgical options. The advantage is that it can verify, complement, or modify the preoperative clinical diagnosis on the one hand, and determine the pathologic stage of gastric cancer on the other.
This pathological examination includes the volume of resected tumor, histologic type, depth of infiltration, presence of intravesical cancer thrombus, lymph node involvement and status, presence of residual cancer cells at the cut edge, and presence of tumor implantation in the outermost plasma membrane of the gastric wall. The pathological findings of the specimens obtained by this route are important for the determination of current and subsequent treatment options for gastric cancer.
Diagnostic surgical resection
Diagnostic surgical resection route refers to the removal of some or all of the diseased tissue for diagnostic purposes for pathologic examination. It is generally used in patients with a clear preoperative pathologic diagnosis and a well-defined surgical plan, and its primary purpose is to determine patient outcome. For example, to determine the nature of the lymph node enlargement, the surgeon will remove the lymph nodes for pathologic examination, which is often an important tool to determine the histologic type of metastatic cancer.
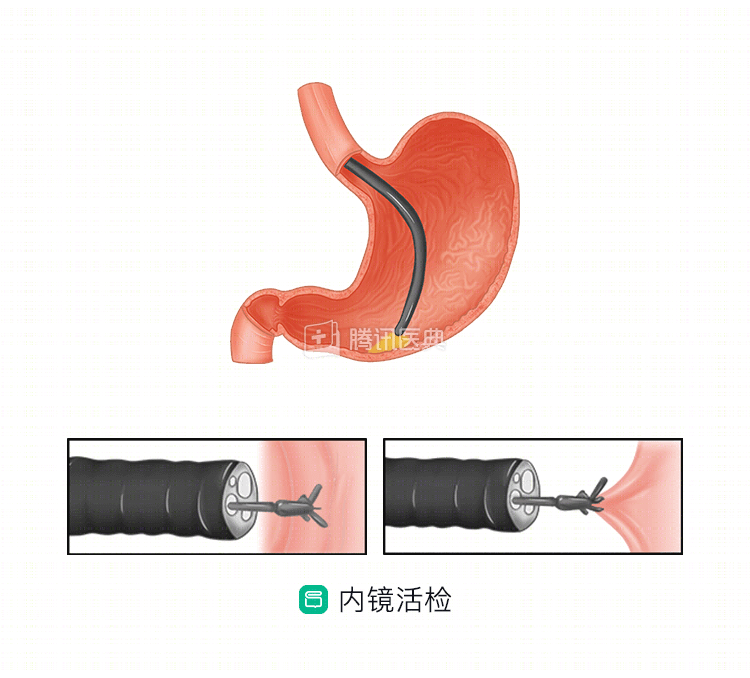
Endoscopic biopsy
With the widespread use of endoscopy, especially fiberoptic endoscopy, physicians are able to obtain biopsies from an increasing number of internal organs for pathologic examination. In gastric cancer diagnosis and treatment, endoscopic biopsy has become a routine tool for preoperative pathological diagnosis.
How do physicians obtain cell specimens?
Cytopathology is a smear examination of cells obtained by natural shedding, scraping, or puncture of the lesion. The advantages over histopathology are that it is less invasive to the patient, cheaper, faster, and usually has a higher positive rate, making it more appropriate for large-scale cancer screening. For gastric cancer diagnosis, the main ways to obtain cellular specimens are as follows.
Intragastric exfoliated cells
Exfoliative cytology is primarily a smear examination of cells that are naturally shed from the lesion. In patients with suspected gastric cancer, fresh exfoliated cells of the gastric mucosa can be obtained from gastric fluid by brushing, washing, and blotting under gastroscopy, and then observed under a microscope after specific staining. The presence or absence of malignant tumor cells can be clarified by this method, which is suggestive for the diagnosis of gastric cancer.
Peritoneal lavage
For the presence of free cancer cells in the abdominal cavity, they can be found by lavage of the abdominal cavity. Usually, before starting radical gastric cancer surgery, the surgeon will inject an amount of 37°C physiologic saline into the perigastric region of the abdominal cavity, slowly stir it up and aspirate it, repeat the lavage 3 to 6 times, and then leave some of the lavage fluid for examination. For those with ascites, the doctor will also directly extract the ascites for examination. Abdominal free cancer cell examination is important in predicting peritoneal metastasis and survival.
Circulating tumor cell assay
Circulating tumor cells are tumor cells that are shed from the primary tumor site and enter the bloodstream. As blood flows through the body, most of the circulating tumor cells will apoptosis or phagocytosis, and only a few will eventually colonize distant organs, leading to distant metastasis. The circulating tumor cell test has the advantages of being easy to obtain, less invasive, and can be performed by blood sampling, and can be used to monitor patients dynamically. The compliance of patients with this test is good. Circulating tumor cell testing carries more comprehensive genetic information, and by combining it with other tests, it can reduce the false-positive rate of gastric cancer, help in the early diagnosis and prognosis of gastric cancer, guide the development of individualized treatment plans, and evaluate the effectiveness of treatment.
Both biopsy histopathology and cytopathology are important tools to diagnose gastric cancer. Doctors will choose the appropriate route to obtain specimens according to the patient’s specific situation, and sometimes may combine multiple means to obtain multiple specimens for a combined pathological diagnosis. (Contributed by Jianhua Wu, Department of Gastrointestinal Oncology, The First Affiliated Hospital of China Medical University)