Radiofrequency ablation is a treatment modality that relies on energy to kill the tumor but not to remove it. The equipment for radiofrequency ablation consists primarily of an alternating current generator and a probe to deliver the energy, and of course the technique of placing the probe through radiology or laparoscopy.
Treatment principles
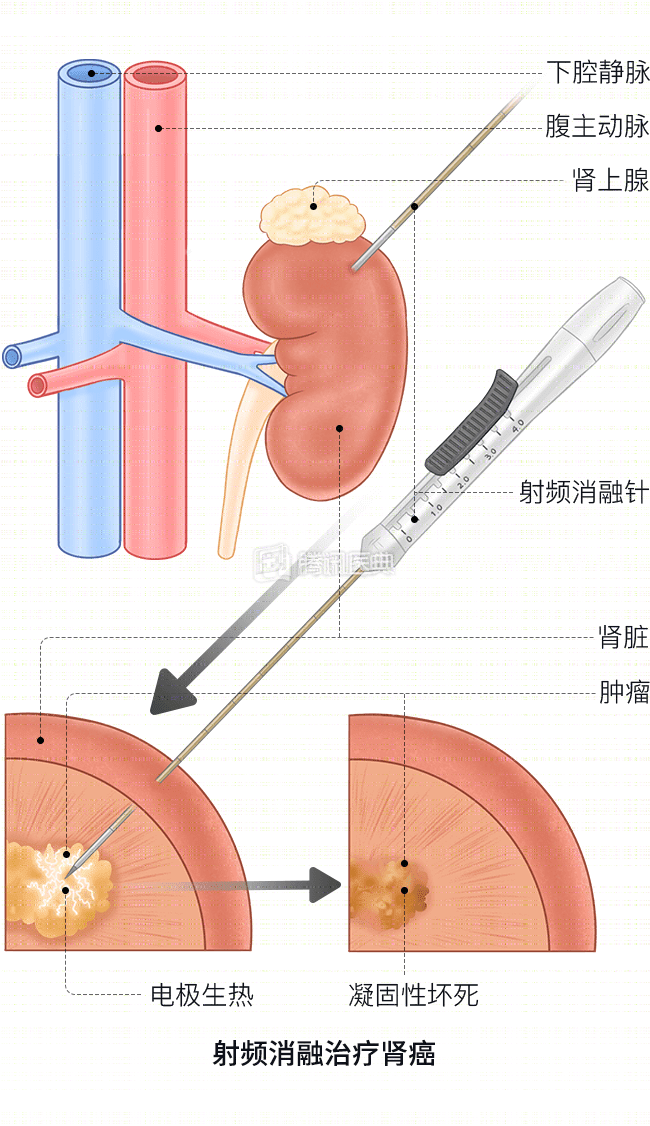
With imaging (CT, ultrasound, etc.) guidance, the radiofrequency energy probe is inserted into the kidney tumor, and the high-frequency radiofrequency waves generated by the radiofrequency generator send radiofrequency currents through the electrodes inserted into the tumor tissue, which then form a circuit through the auxiliary electrodes, generating heat through molecular friction and ion escape in the surrounding tissue, resulting in coagulative necrosis of the tumor tissue at local temperatures of up to 90-100°C.
The main mechanisms of radiofrequency ablation for tumor treatment include:
- High temperature causes coagulative necrosis of tumor tissue in the target area and directly kills tumor cells;
- High temperature affects various functions of the cell membrane, leading to apoptosis;
- High temperature increases the activity of lysosomal enzymes in tumor cells and affects the normal function of many organelles, especially mitochondria;
- High temperature causes coagulation of vascular tissues around the tumor, forming a reaction zone, thus reducing or blocking tumor blood supply and preventing tumor spread;
- During the coagulation necrosis of tumor cells, antigen exposure at cell membranes and other sites or changes in the immune phenotype of tumor cells can stimulate the body to produce specific antibodies to kill or inhibit tumor growth or spread, which is known as “endogenous tumor seeding”, making tumor cells easier to be recognized and killed by the body’s immune cells.
Population
Radiofrequency ablation technology is mainly used for patients with kidney cancer who are inoperable, cannot tolerate surgery and refuse surgery. For example, elderly patients, isolated kidney, patients with other serious diseases (such as coronary heart disease, diabetes mellitus, chronic obstructive pulmonary disease, etc.), patients with renal insufficiency, certain hereditary diseases (such as hereditary papillary renal cancer), etc.
Efficacy
The radiofrequency ablation devices currently in clinical use can produce foci of local coagulative necrosis of 1 to 5 cm in diameter, so small renal cancers are more suitable for radiofrequency ablation. The success rate of 1 or more ablations for cancers less than 3 cm in diameter is 92% to 100%, and cancers larger than 4 cm in diameter often cannot be completely ablated in 1 treatment and require 2 or more ablations.
In addition, the location of the tumor directly determines the efficacy of radiofrequency ablation. The exophytic type is easier to puncture than the central type, and the insulating effect of the perirenal fat capsule can bring the tumor tissue to a higher temperature during radiofrequency emission and maintain it for a long time, so the ablation effect is better; whereas the central type is close to the large blood vessels in the hilum, and the “thermal deposition” effect generated by the blood flow partially cools the tumor tissue. The “thermal deposition” effect partially cools the tumor tissue, thus limiting coagulative tumor necrosis, and there is a greater risk of bleeding during treatment of central-type renal cancer.
Side effects
The most common complications of radiofrequency ablation are bleeding, hematuria, and perirenal hematoma, but all are mild and do not require special management. Central renal cancer has a higher risk of bleeding, which can break into the collecting system of the kidney.
- If the clot obstructs the collecting system it will lead to urinary tract obstruction;
- If ureteral injury leads to ureteral stricture or urinary leakage.
In addition, there is injury to the lumbar plexus or genitofemoral nerve leading to pain and loss of sensation in the skin of the groin.
Patients who notice hematuria, difficulty urinating, or severe pain after surgery should talk to their primary care physician to avoid serious complications.