In one forum, many young people post that they suspect they have esophageal cancer, describing the same symptoms as the common manifestations of esophageal cancer, and the more they look, the more they look, the more worried they become. The more you search for information on the Internet, the more distressed or anxious you will be, which is closely related to “hypochondria”.
But today we’re not talking about “hypochondria,” but rather about the atypical symptoms that lie behind esophageal cancer and the “remedies” to get rid of them.
Is it possible to have esophageal cancer in your 20s?
Can you get esophageal cancer in your 20s?
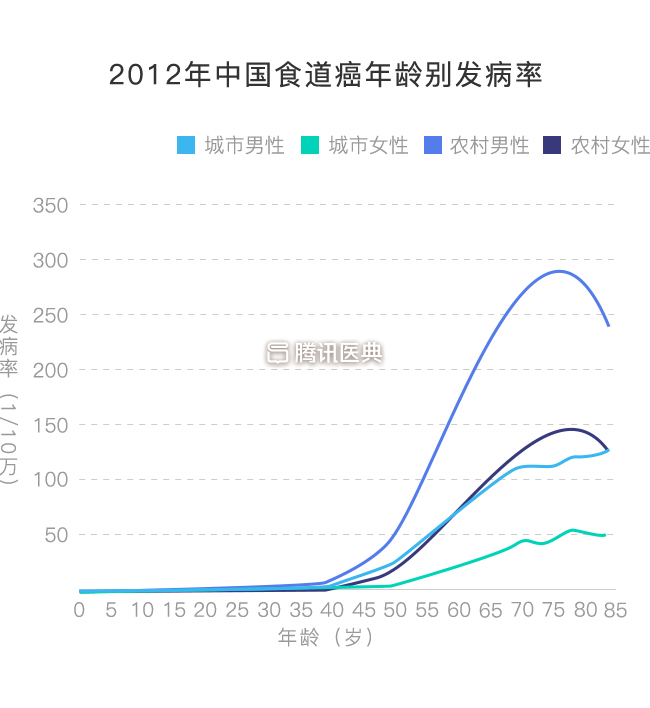
How high is the risk of esophageal cancer in teenagers and young adults in their 20s? To relieve esophageal cancer anxiety, let’s first look at how old the high incidence age is.
Studies have found that the incidence of esophageal cancer is at a low level until age 40; it begins to rise rapidly after age 40. In addition to rural men, both rural women and urban populations, their esophageal cancer incidence peaks in the 80-year-old age group and declines after age 85 (shown in the chart below). The incidence of esophageal cancer in young people in their 20s is a bit of a “worry in the dark”.
While young people are not as likely to get esophageal cancer, it is important to be careful if you have an older family member who has had esophageal cancer or other cancers. Esophageal cancer is not directly inherited, but having a family history of cancer may increase a person’s risk of developing esophageal cancer.
For example, in areas of China with a high incidence of esophageal cancer (such as Lin County, Henan Province), 25% to 50% of people with esophageal cancer have had a relative in their family who has had cancer.
With these symptoms, could it be esophageal cancer?
Hiccups, cough, frequent choking on food, constant phlegm in the throat, dry throat, always having something blocking it, pain in the saber position in the back, swelling and pain behind the sternum, and a feeling of foreign body blockage …… These manifestations can occur at different times in esophageal cancer, but are more common in other benign diseases.
● For example, cough is a common manifestation of colds, pneumonia, bronchitis, etc.; heartburn, acid reflux, burping, nausea after eating, and gas and bloating are common symptoms of acid reflux.
What to do if you have difficulty swallowing? Instead of fear and anxiety and sleeplessness, it is better to seek early medical attention to identify the cause.
Difficulty swallowing is not unique to esophageal cancer. Chronic pharyngitis, esophagitis, esophageal diverticula, esophageal varices, cardia loss, and other benign diseases may cause dysphagia.
In addition, symptoms due to esophageal cancer tend to be persistently worse compared to dysphagia due to benign disease. That is, the discomfort manifests itself more severely over time.
So, in most cases, dysphagia in young people is a benign esophageal or gastric condition and is not something to be overly concerned about. However, once you pass middle age, you need to be more alert to these atypical manifestations.
There are three steps to diagnose esophageal cancer in time
The best way to relieve anxiety about “esophageal cancer” is to go to the hospital.
Barium meal
Regardless of age, if esophageal cancer or esophageal disease is suspected, barium gastrointestinal imaging is the most basic imaging method to examine esophageal lesions. The test is also known as a “barium meal” because of the white barium sulfate contrast agent that is drunk before the test.
● Barium reaches the stomach and duodenum via the esophagus, making a shadow along the way to diagnose upper gastrointestinal tract disease, and is a noninvasive test. The hospital’s imaging physician will make a preliminary clinical diagnosis based on the imaging performance of the upper gastrointestinal contrast examination.
Gastroscopy
If the barium meal is inconclusive, the next step is a gastroscopy.
● Electronic gastroscopy is an important diagnostic method for esophageal cancer, in which a miniature camera “videos” your esophagus and stomach and displays them clearly on a monitor for your doctor to see. However, what is seen under the gastroscope cannot accurately determine the early or late stage of the disease. Because the gastroscope cannot see the depth of infiltration of the mass, it can only see the internal manifestations of the esophagus, such as new organisms (see below). The exact staging still requires a pathology biopsy to be taken for diagnosis.
Pathologic biopsy of esophageal cancer is usually obtained during gastroscopy using biopsy forceps to obtain lesion tissue. The vast majority of samples sent for examination will yield a definitive histopathologic diagnosis. The pathologist will determine if it is cancer and the type and differentiation of the cancer based on the morphology and distribution of the diseased tissue cells under the microscope.
Tumor markers
Sometimes, your doctor may also send you for a blood draw to check for tumor markers.
● Tumor markers are substances that are present in, or produced by, tumor cells during tumor proliferation, or can be produced by the body in response to tumor stimulation.
Although, there are no particularly reliable tumor markers for esophageal cancer, combined testing of two or more markers can be meaningful for diagnosis or screening. Possible markers of choice include: carcinoembryonic antigen (CEA), glycoantigen CA72-4, glycoantigen CA19-9, squamous cell carcinoma-associated antigen (SCC), and cytokeratin 21-1 (Cyfra21-1).
The symptoms of choking, throat discomfort, uncomfortable swallowing, and foreign body blockage are really easy to “pinpoint” to esophageal cancer. The company’s main goal is to provide a comprehensive range of products and services to the public. The company’s main goal is to provide the best possible service to its customers.
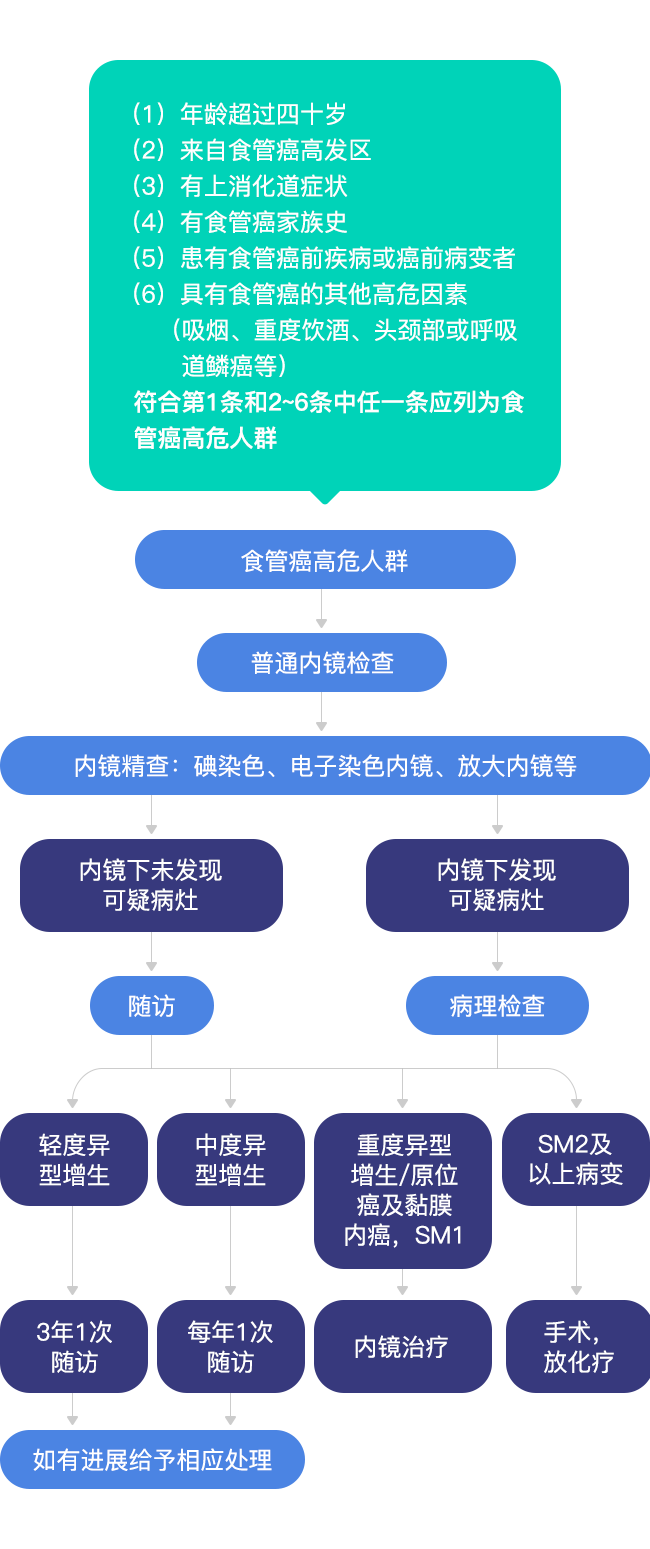
Finally, a flow chart of early esophageal cancer screening and endoscopic precision is attached, and it is recommended to focus on collecting it if you are one of the high-risk groups described in the chart below.