Key points of this article:
- Bone metastases from prostate cancer can lead to serious consequences such as bone pain, fractures, and even paraplegia, and the progression is relatively insidious and not easily detected, making early detection and control of bone metastases very important.
- ECT is the most sensitive test for diagnosing bone metastases, detecting them earlier than conventional X-rays, and is recommended routinely for patients with prostate cancer.
- ECT reflects bone formation.
- ECT reflects functional changes in bone formation and blood flow, whereas X-rays only show morphologic changes.
- ECT looks at the whole body, whereas X-rays can only look at symptomatic localized areas; therefore, there is a risk of missing occult lesions on X-rays.
- ECT can detect early osteogenic changes, whereas X-rays can only detect abnormalities when bone destruction is greater than 50%.
- Advanced bone metastases are in an inactive stage, and ECT may be negative and fail to detect the lesion, while X-rays show significant bone destruction.
- Class I: Prognosis is good for primary prostate cancer, with a single bone metastasis and more than 3 years between the discovery of the primary site and the appearance of the bone metastasis.
- Class II: Pathologic fracture of major long bones (humerus, ulna, radius, femur, tibia, and fibula are long bones).
- Class III: Imaging or clinical signs of an impending pathologic fracture of the major long bones or around the acetabulum.
- Class IV: multiple osteogenic metastases, osteolytic or mixed metastases on non-weight-bearing bones (e.g., fibula, ribs, sternum, clavicle, etc.), osteolytic lesions on major long bones without a temporary risk of fracture, lesions located on the iliac wing, anterior pelvis, or scapula (excluding patients in Class I).
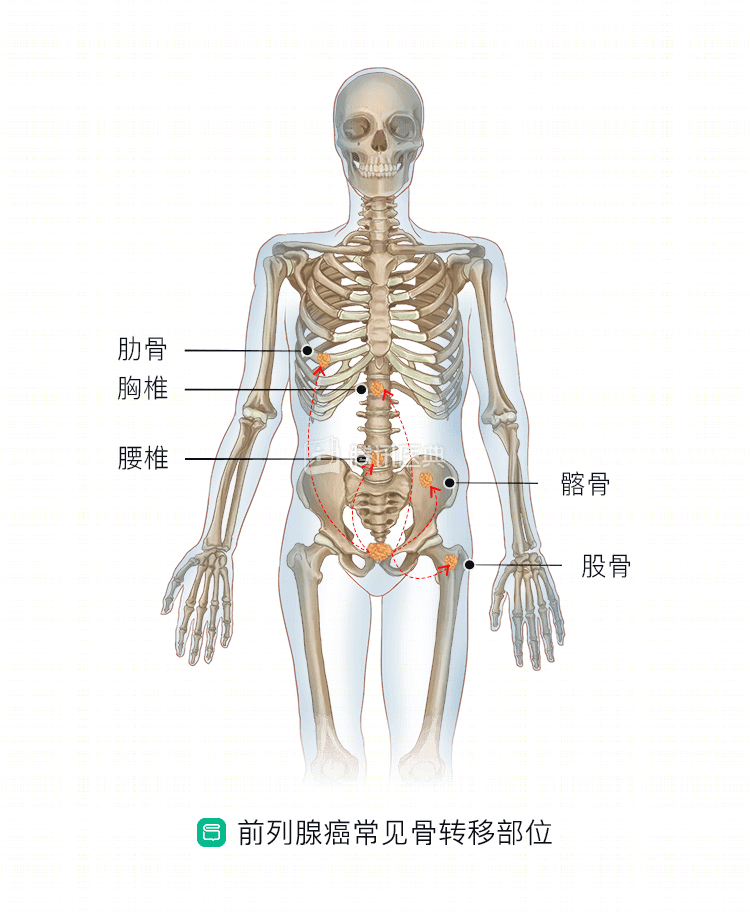
Bone metastases from prostate cancer can occur in any bone, and the common sites for bone metastases are the pelvis, lumbar spine, sacrum, thoracic spine, and ribs. In general, the less differentiated the cancer, the higher the chance of skeletal metastases.
Most patients with bone metastases from prostate cancer develop insidiously, and when the metastases trigger symptoms, the most common presentation is pain, which usually develops confined and intermittently, gradually worsens, and after weeks to months, develops into severe pain, especially at night. The pain is especially pronounced when the patient is lying down, and in severe cases, pathological fractures or paraplegia may occur.
Prostate cancer patients with bone metastases have a worsening of their general condition in advanced stages, with loss of appetite, lethargy, anemia, and even cachexia in some cases. The most important thing is to make sure that you have a good understanding of the situation.
At present, bone metastases from prostate cancer are diagnosed by the following methods:
1. ECT nuclide bone imaging
ECT (emit computed tomography) is the most sensitive test for diagnosing bone metastases, and it can detect bone metastases 3-6 months earlier than conventional X-rays.
The contrast agent for ECT is 99mTc-methylenediphosphonate (MDP), which is able to visualize the lesion because the radionuclide selectively concentrates in the reactive new bone formation zone of the tumor, as evidenced by increased uptake (concentrated/hot zone) or decreased uptake (cold zone). The “super bone image” and “headless bone image”, in which radionuclide uptake is diffusely increased throughout the skeleton, are most commonly seen in prostate cancer metastases.
The sensitivity of ECT for detecting bone metastases is about 96.3%, which is close to that of MRI, and can be detected on bone scan when the metastases are not less than 2 mm in diameter and have metabolic changes (5% to 15%), 1 to 6 months earlier than on X-ray. However, the drawback is the relatively low specificity of detection (66.7%) and the high false-negative rate for lesions in the spine and confined to the bone marrow, which is more typical when metastases are confined to the medulla and do not invade the cortex.
2. Bone radiographs
The sensitivity of bone radiographs for the diagnosis of bone metastases is low, about 48.1%, and metastases need more than 50% bone destruction and 1.0 to 1.5 cm in diameter to be detected. Bone X-rays detect bone metastases later than whole-body ECT and are not routinely used for further evaluation of abnormalities at symptomatic sites (e.g., pain, pathologic fractures) or on other imaging studies (e.g., whole-body bone imaging and MRI).
In addition, about 25% of prostate cancer patients with normal bone X-rays (no bone metastases) have signs of bone metastases after ECT, suggesting that X-rays are less reliable than ECT in detecting early bone metastases.
While the sensitivity of bone X-rays is extremely low, they have the advantage of being relatively specific, at 94.4%, and show certain features of bone metastases that can help distinguish them from other lesions or primary bone tumors.
ECT vs bone radiographs
Let’s summarize our comparison of ECT and radiographs:
In conclusion, ECT is an effective systemic test for bone metastases. x-ray is less sensitive and is of greater diagnostic value when ECT is positive and inconclusive, and the combination of ECT and x-ray significantly reduces the false-positive rate and increases the specificity, making the diagnosis of bone metastases more reliable.
In addition, CT and MRI are reliable methods for those with suspicious ECT but inconclusive X-rays.
3. Other tests
PET has high specificity but low sensitivity and is expensive for the diagnosis of bone metastases. Although CT-guided bone aspiration biopsy has improved safety, it is still an invasive test; also, bone metastases from prostate cancer are often multiple foci, so these two diagnostic methods are not routinely recommended.
In addition to these methods, there are laboratory tests that can be suggestive, such as blood alkaline phosphatase and blood calcium, which are usually elevated.
Pathologic diagnosis is still the gold standard for diagnosing bone metastases, especially for patients with prostate cancer who present with a single foci of bone destruction, and when the diagnosis is not clear, a bone biopsy can be performed to obtain bone tissue for pathologic examination to accurately determine whether there are bone metastases from prostate cancer.
After diagnosis, if bone metastases do exist, doctors often classify prostate cancer bone metastases into the following 4 categories:
Bone metastases are classified into different types because the treatment varies between patient categories.
Related articles: