Bone marrow aspiration
Bone marrow is a spongy tissue present in the marrow cavity of long bones (e.g., humerus, femur), the cancellous interosseous mesh of flat bones (e.g., sternum, ribs) and irregular bones (ilium, vertebrae, etc.), and is the main organ of human hematopoiesis.
Puncture is a common diagnostic technique for taking bone marrow fluid, and its examination includes several aspects of cytology, protozoa, and bacteriology. It is indicated for:
- Diagnosis, differential diagnosis and therapeutic follow-up of various hematologic diseases;
- Unexplained increased or decreased red blood cell, white blood cell and platelet counts and morphological abnormalities;
- Diagnosis and differential diagnosis of unexplained fever, with the possibility of bone marrow culture and bone marrow smear to look for parasites, etc.
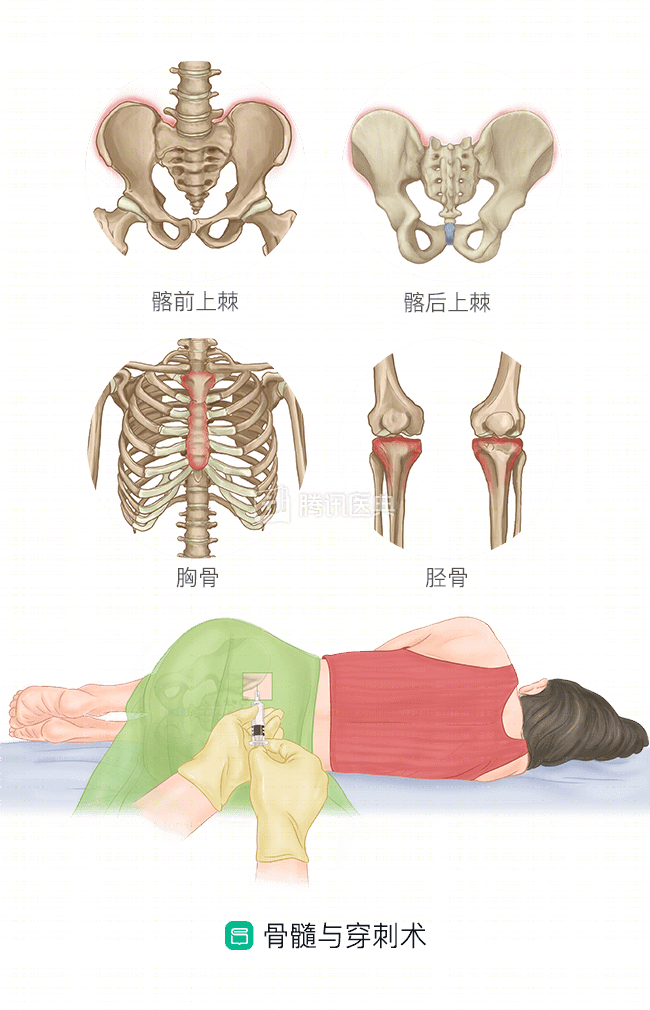
Specimen collection is usually taken from the anterior and posterior superior iliac spine, and in a small number of patients, the sternal area is required.
The bone marrow contains mainly the granulocyte system (including neutrophils, eosinophils, and basophils), the erythroid system, the megakaryocyte system (platelet-producing cells), the lymphocyte system, the monocyte system, and a very small proportion of nonhematopoietic histiocytes. The diagnosis can be made by bone marrow cell smear and pathological examination, respectively.
Bone marrow smear
Bone marrow smear is performed by aspirating 0.2 ml of bone marrow fluid and applying it to a single cell layer on a slide, usually through an oil microscope (magnification 1000x), to observe the specific morphology and internal structure of the cells, the degree of proliferation and the ratio of various cells, and the presence of abnormal cells and parasites.
- Bone marrow proliferation is classified into five grades – extremely low, low, active, markedly active, and extremely active. The degree of proliferation in normal bone marrow is active to markedly active.
- The normal ratios and proportions for each cell system and each stage are as follows.
- The granulocyte lineage occupies 40-60% of the nuclei, with progranulocytes <2% and early juvenile granulocytes <5%, with increased cells in later stages and rod nuclei > lobulated nuclei.
- The erythroid lineage is actively proliferating, occupying approximately 20% of the nuclei, with proerythrocytes <1% and early juvenile erythrocytes <5%, and predominantly middle to late juvenile erythrocytes, each accounting for approximately 10%.
- Granulocytes: erythrocytes = 2 to 4:1.
- The lymphocyte lineage accounts for about 20% of the nucleated cells, and up to 40% of the mature lymphocytes in young children; primary and juvenile lymphocytes are rare.
- Monocyte and plasma cell lineages: <4% monocyte lineage and <2% plasma cell lineage, both of which are predominantly mature cells.
- Megakaryocytic lineage: the number of megakaryocytes in the whole film is about 7-35, platelets are in groups of 3-5, and there is one platelet for an average of 25 red blood cells.
- Other cells are rare.
- Other cells are rare.
- Aberrant cell morphology will also be described specifically for each stage, as well as for other sources of abnormal cells, parasites, etc.
If abnormal manifestations are present, they can be interpreted as follows:
The degree of bone marrow proliferation:
- Extreme hypoproliferation: seen in patients with typical aplastic anemia, or other hematopoietic failures, etc.
- Decreased proliferation: seen in chronic aplastic anemia and very rarely in hypoproliferative leukemia, when the bone marrow is suppressed during chemotherapy for tumors, leukemia, etc.
- Actively proliferating: seen in healthy individuals, diseases not primary to the hematopoietic system and early lymphoma, multiple myeloma, hematologic disorders that have not yet developed disorders of the hematopoietic system, and a few atypical leukemias, anemias, and bacterial infections.
- Significantly active hyperplasia: seen in all types of hyperplastic anemia, such as iron deficiency anemia, hemolytic anemia, megaloblastic anemia, and acute blood loss, bone marrow reactions to drugs or biologics, bacterial infections, atypical acute and chronic leukemia, myeloproliferative disorders, hypersplenism (hypersplenism can cause increased phagocytosis of blood cells by the spleen) (hypersplenism can cause increased phagocytosis of blood cells by the spleen, resulting in a decrease in blood cells and thus a proliferation of myeloid cells), etc.
- Extremely active hyperplasia: seen in all types of typical acute leukemia, chronic leukemia, and various myeloproliferative disorders, as well as in subjects treated with certain biologically active agents.
A simple determination can also be made for the increase or decrease in the ratio of cells in each lineage:
- Granulocyte lineage
- increased – progranulocytic (acute leukemia, etc.), early juvenile (acute promyelocytic leukemia), intermediate juvenile (partially differentiated acute granulocytic leukemia, chronic granulocytic leukemia, etc.), late juvenile and rod-shaped nuclei (chronic granulocytic leukemia, leukoid, toxic, etc.);
- Decreased – aplastic anemia, granulocyte deficiency, acute hematopoietic arrest, etc.
- Red blood cell lineage
- increased – proerythrocytic and early juvenile red (acute erythroleukemia, acute erythroleukemia), intermediate and late juvenile red (proliferative anemia, true erythrocytosis, lead poisoning, erythroleukemia, etc.);
- Decreased – pure red cell aplastic anemia, acute leukemia undifferentiated type, post-chemotherapy, etc.
- Megakaryocytic lineage
- increased – idiopathic thrombocytopenic purpura, acute megakaryocytic leukemia, hypersplenism, chronic granulocytic leukemia, etc.
- Decreased – aplastic anemia, chronic granulocytic leukemia, post-chemotherapy, etc.
- Monocyte lineage
- increased – promonocytic and juvenile monocytes (acute monocytic leukemia, acute granulocytic-monocytic leukemia, chronic granulocytic leukemia acute monocytic transformation), mature monocytes (acute red leukemia, acute red leukemia)
- Lymphocytic lineage
- increased – prolymphatic and juvenile lymphatic (acute lymphoblastic leukemia, acute lymphoblastic transformation of chronic granulocytic leukemia, lymphoma, etc.), mature lymphatic (chronic lymphoblastic leukemia, lymphoma, macroglobulinemia, aplastic anemia, viral infections, etc.)
Myelopathologic diagnosis
Bone marrow pathology is diagnosed by extracting 2 cm of bone tissue, which is processed by HE staining and immunohistochemistry and analyzed under high magnification (200-400x magnification). It helps to provide an overall understanding of the ratio of red (hematopoietic tissue) to yellow (adipose tissue) bone marrow (generally 50:50, but red marrow is physiologically reduced in the elderly), and the cellular composition within the bone marrow, and it maintains the structure of the bone marrow trabeculae, and malignant cells are easier to recognize for pathologic diagnosis.
The diagnosis of some diseases requires knowledge of bone marrow histology, such as aplastic anemia, myelofibrosis, myelodysplastic syndromes, and bone marrow metastases from malignant tumors requires bone marrow pathology.
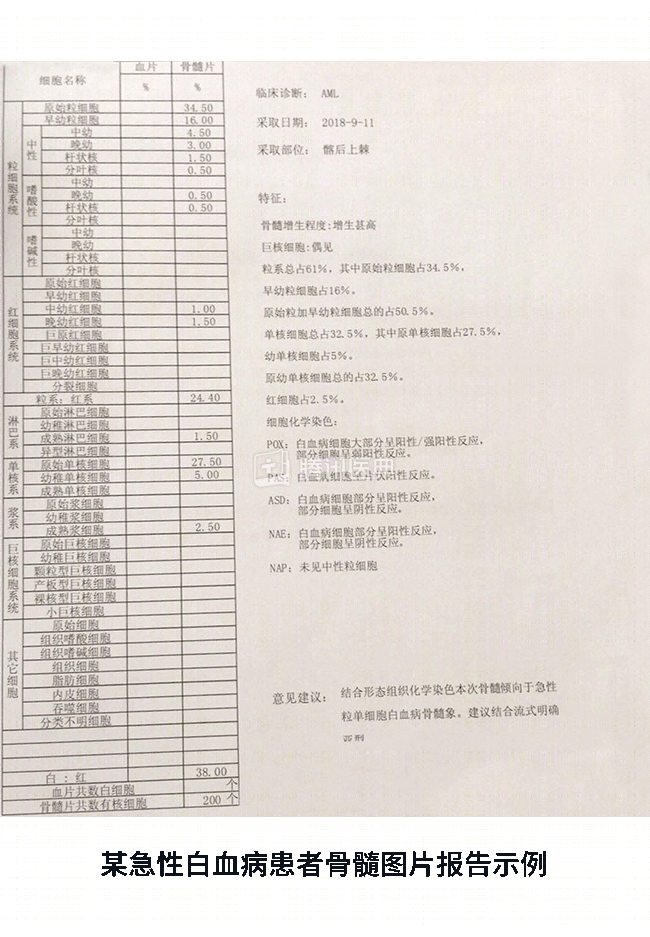
However, the results of the bone aspiration report need to be combined with all the indicators to make a comprehensive judgment. In the case of acute leukemia, as shown in the accompanying figure, a bone marrow smear from a patient needs to be combined with MICM (morphology, immunology, cytogenetics, molecular biology) to make a definitive diagnosis. When the bone puncture report is available, it is still recommended that a comprehensive diagnosis be made under the guidance of a medical professional.