How is stage I medullary thyroid cancer treated? We present the experiences of two patients to help clear up your doubts.
Case 1
Ms. Li, 45, had a right-sided thyroid nodule (about 1.5 cm) found on ultrasound at her workplace, and her relatives had no history of thyroid cancer.
The doctor recommended a fine-needle aspiration biopsy, which suggested “suspicion of medullary carcinoma”. The blood was drawn: thyroid function was normal, serum calcitonin and carcinoembryonic antigen (CEA, a tumor marker) levels were significantly elevated, and there were no abnormalities on adrenal ultrasound.
After hospitalization, Ms. Li underwent “bilateral thyroidectomy + lymph node dissection in the right VI region” after completing thyroid CT, electrocardiogram, lung function, and chest radiographs to rule out contraindications to surgery. The postoperative pathology suggested that medullary carcinoma of the right thyroid gland without extraglandular invasion or lymph node metastasis; stage: T1N0M0 (tumor confined to the thyroid gland, maximum diameter not larger than 2 cm; no lymph node metastasis or distant metastasis).
Ms. Li is recovering well from surgery and has been discharged from the hospital. She takes 1 oral levothyroxine tablet daily and is being reviewed regularly without further radiation or chemotherapy.
Case 2
Mr. Wang, 36 years old, was seen on physical examination for bilateral thyroid nodules (1.5 cm on the left and 1 cm on the right), and his mother had medullary thyroid cancer.
The doctor recommended the following tests: fine needle aspiration biopsy, thyroid function and serum calcitonin, carcinoembryonic antigen CEA, thyroid CT, and adrenal ultrasound. The results showed bilateral medullary thyroid carcinoma with bilateral adrenal pheochromocytoma. The doctor recommended treating the adrenal pheochromocytoma first and then elective surgery for thyroid cancer when the disease stabilized.
After surgery for adrenal pheochromocytoma and stabilization, the surgeon performed “bilateral thyroidectomy + bilateral VI lymph node dissection”. The postoperative pathology showed bilateral medullary thyroid carcinoma without extraglandular invasion and lymph node metastasis; stage: T1N0M0.
Mr. Wang recovered well.
Mr. Wang has recovered well and has been discharged from the hospital. He takes 1 tablet of oral levothyroxine daily and has regular follow-ups without radiation or chemotherapy. The doctor advised his first-degree relatives (close siblings, parents, and children) to have timely thyroid physicals and genetic counseling.
What is the basis for the doctor’s treatment?
Medullary thyroid cancer is classified as familial or sporadic, and they are treated differently. How did the doctors make the choice of treatment for these two patients? The most recent National Comprehensive Cancer Network (NCCN) guidelines are currently used by doctors in China and are summarized below:
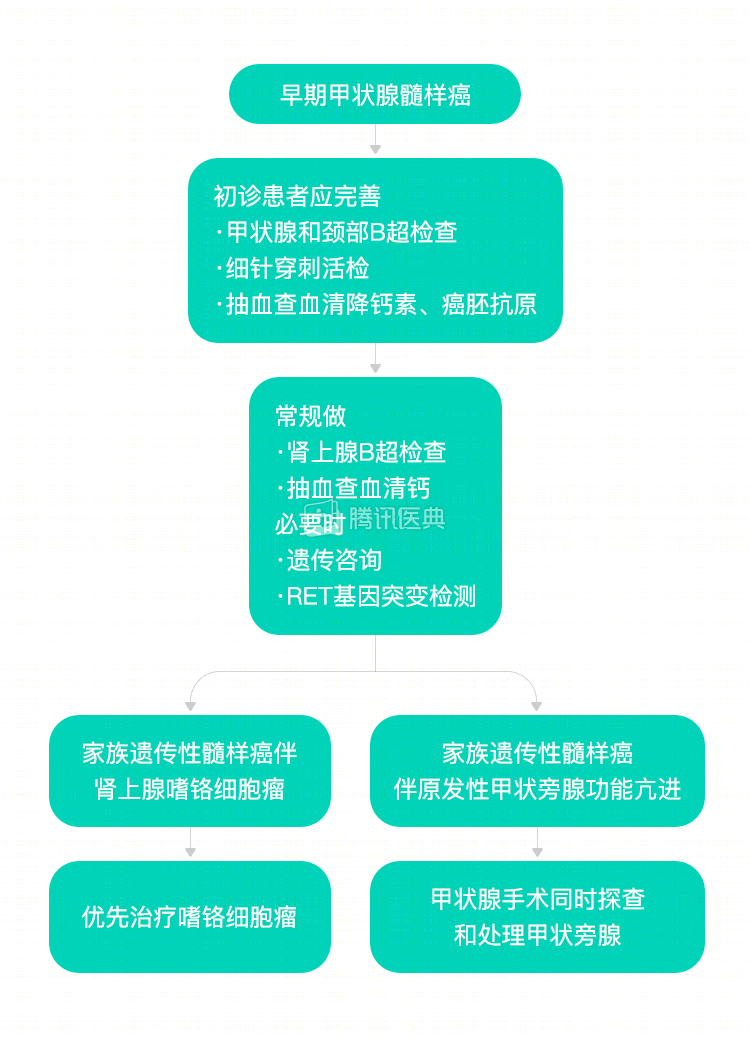
Bilateral thyroidectomy + lymph node dissection in the VI region of the disease is recommended for stage I medullary carcinoma, followed by levothyroxine tablets without radiotherapy or chemotherapy.
Frequently asked questions about the management of early medullary thyroid cancer
.
Is there a high incidence of medullary thyroid cancer?
The incidence is low, accounting for only 5% of all thyroid cancers.
How do I know if a thyroid nodule is benign or malignant? If it is malignant, how do you rule out medullary carcinoma?
The first choice for determining whether a nodule is benign or malignant is thyroid ultrasound, which in combination with fine needle aspiration can greatly improve diagnostic accuracy.
Puncture can usually determine if the tumor is medullary, which is also characterized by elevated serum calcitonin and carcinoembryonic antigen (CEA), both of which can further confirm the diagnosis.
What is hereditary myeloid carcinoma? What is sporadic myeloid carcinoma?
What is hereditary myeloid carcinoma?
Hereditary myeloid carcinoma is a condition in which multiple people in the same family have the disease at the same time or in succession, usually with a mutation in the RET gene. If this is not the case, the patient has sporadic myeloid cancer. Sporadic myeloid carcinoma accounts for about 75% of all myeloid carcinomas.
How do I know if I have hereditary or sporadic myeloid cancer? Does my loved one need genetic testing?
If you have medullary thyroid cancer, how can you tell if it is hereditary or sporadic? First, your doctor will ask you in detail if any of your first-degree relatives (parents, siblings, and children) have medullary thyroid cancer; second, you can go to a medical professional to test for the RET gene mutation.
First-degree relatives of patients with medullary thyroid cancer are currently recommended to have their thyroid and adrenal glands examined and, if available, tested for RET mutations at a regular hospital.
Do all patients with hereditary medullary carcinoma develop pheochromocytoma? Why is it important to treat pheochromocytoma first? Will it delay treatment of myeloid cancer?
There are three main types of hereditary medullary carcinoma: multiple endocrine neoplasia type 2A (MEN2A), multiple endocrine neoplasia type 2B (MEN2B), and familial medullary thyroid carcinoma (FMTC). Of these, MEN2A is the most common, accounting for 95% of all hereditary medullary carcinomas. the incidence of pheochromocytoma in patients with MEN2A and MEN2B is 42% and 40%, respectively; FMTC is not associated with pheochromocytoma.
Adrenal pheochromocytoma can cause paroxysmal hypertension, and thyroid surgery first may precipitate hypertensive crisis or heart failure, so the pheochromocytoma should be removed first. This will not delay treatment of medullary carcinoma.
Why should Ms. Lee in case 1, who has no family history of medullary carcinoma, also be screened for pheochromocytoma?
There are two reasons. First, patient dictation does not always reflect the true picture, and Ms. Li may have a first-degree relative with unrecognized medullary carcinoma. Second, Ms. Li may be the first person in her family to develop the disease. The author’s center recommends routine adrenal ultrasound for all patients with medullary carcinoma.
Do I need radiation or chemotherapy after surgery for stage I medullary thyroid cancer?
Surgery is preferred for stage I medullary thyroid cancer without extrathyroidal invasion and lymph node metastases, and radiation or chemotherapy is usually not needed for patients who are not assessed by their physicians to have high-risk factors for recurrence.
How do I take levothyroxine tablets after surgery for medullary carcinoma?
After surgery to remove the whole thyroid gland, you need to take levothyroxine tablets for life after surgery to supplement the postoperative thyroid hormone deficit. If only one side of the thyroid gland was removed, it is usually necessary to stop taking it for 3 months after surgery and then stop after 1 month when thyroid function is normal.
Take the medication daily in the morning on an empty stomach, and adjust the dose according to thyroid function tests to maintain thyrotropin (thyroid stimulating hormone TSH) and thyroid hormones (T3 and T4) in the normal range. If you are pregnant, dose adjustments will require consultation with your obstetrician.
Disclaimer:
Tumor disease and treatment options are extremely complex, and treatment should be fully individualized, and this case does not represent a “like patient” treatment decision. Please seek professional advice from a competent physician regarding your specific treatment plan.
Co-written by Dr. Ben Ma, Fudan University Cancer Hospital