1. Pre-treatment evaluation
Before radiotherapy, a detailed examination should be performed to clarify the specific condition of the tumor and to prepare for the target area: hoarseness, dysphagia and wheezing indicate that the tumor has invaded the thyroid body and reached the laryngeal nerve, esophagus and trachea. Detailed examination of the neck for enlarged lymph nodes to determine whether there is regional lymph node metastasis. Laryngoscopy will be performed to determine whether there is vocal cord paralysis and whether there is invasion of the recurrent laryngeal nerve. Ultrasound and CT of the neck can be used to clarify the extent of tumor invasion and enlarged lymph nodes in the neck; CT of the lung, ultrasound of the abdomen and bone scan should be routinely examined to exclude the possibility of distant metastasis. Before postoperative radiotherapy, detailed information about the operation, postoperative residual and postoperative pathological results should be obtained.
2. Radiotherapy techniques
Conformal radiotherapy or conventional radiotherapy can be used.
(1) Intensity-modulated radiation therapy (IMRT) and three-dimensional conformal radiotherapy.
(1) Simulated CT localization.
Position selection: the best position is supine, with a head frame (to ensure that the head is as supine as possible) and headrest at a suitable angle, and fixed with head, neck and shoulder thermoplastic film. C pillow is generally used in the radiotherapy department of the Cancer Hospital of the Academy of Medical Sciences, which can keep the neck in the hyperextended position. Simulated CT scan: Spiral CT is used for scanning, and all patients should be scanned with iodine contrast for enhancement, with a layer thickness of 3mm, and the upper border should include the cranial vault and the lower border should include all lung tissues; upload to the planning system.
2) Target area development (Figure 4): There is a large controversy regarding target area determination. Some studies believe that small field treatment can be used, with adequate attention to the surgeon’s external radiation to areas of high postoperative incidence, and areas that are not easily resected by surgery. Some investigators believe that large field radiotherapy should be given, with the choice of treating the cervical lymph node drainage area. The design of the target area should be based on the specific circumstances such as the type of pathology, the extent of the lesion, and the presence or absence of lymph node invasion. Generally speaking, small field is used for highly differentiated carcinoma and large field is used for poorly differentiated or undifferentiated carcinoma. In principle, the irradiation field of thyroid cancer should include the entire thyroid body and regional lymphatic drainage, and the upper and lower boundaries should be decided according to the extent of tumor invasion and the extent of lymph node metastasis. For undifferentiated carcinoma, the upper field should include the upper cervical lymph nodes, and the lower field should reach the level of the tracheal bifurcation to include the upper mediastinal lymph nodes.
The current therapeutic field is mostly large field treatment, which needs to include the lymph node drainage area of the neck and upper mediastinum.
A. Tumor bed (GTVtb): including the area of preoperative tumor invasion, and the extent of metastatic lymph node involvement. For those with irregular surgery, the surgical bed should be considered as GTVtb for outlining.
B. High-risk area (CTV1): including the thyroid area, the surrounding lymph node drainage area and all areas with pathologically confirmed positive lymph nodes.
C. Selective treatment area (CTV2): including lymph node drainage areas II-VI without pathological confirmation but with possible metastasis and lymph nodes in the upper mediastinum. The metastasis rate of posterior pharyngeal lymph nodes and lymph nodes in area I is low, but if there is lymph node metastasis in area II, the probability of metastasis of posterior pharyngeal lymph nodes increases significantly, and if there is larger lymph node metastasis in area IIa, the probability of metastasis of lymph nodes in area Ib also increases, which should also be included in the treatment area. The upper border of CTV2 is generally at the level of the mastoid tip and the lower border at the level of the aortic arch (if there is pathologically confirmed lymph node metastasis in the upper mediastinum, the lower border should be appropriately shifted downward).
Figure 4. Typical levels of target area outline for thyroid cancer
3) Prescribed dose (Figure 5).
A. Selective treatment area (or low risk area): 50Gy-54Gy for general administration.
B. Highly suspicious area of involvement: 59.4Gy-63Gy.
C. Area with positive cut edge pathology: 63Gy-66Gy.
D. Naked eye residual area: 66Gy~70Gy.
E. Normal tissue limits: maximum dose of spinal cord ≤ 4000 cGy; average dose of parotid gland ≤ 2600 cGy; maximum dose of larynx ≤ 7000 cGy (no hot spot should appear in the area of larynx).
Figure 5 Typical levels of IMRT dose distribution for thyroid cancer
(2) Conventional radiotherapy techniques.
(1) Positioning: The same position as IMRT is recommended for positioning using simulated CT and outlining the field on the planning system. In the absence of analog CT equipment, X-ray orthogonal images can also be used for outlining the field.
2) Radiographic field design.
A. Two anterior oblique field cross-angle wedge irradiation technique: see Figure 6.

Figure 6 Two anterior oblique field cross-angle wedge irradiation technique
B. Single anterior field irradiation with electron beam (Figs. 7, 8): The appropriate thickness of wax and oil gauze filler is used to ensure a satisfactory dose distribution to the thyroid and cervical lymph nodes, while the spinal cord is in the low dose area.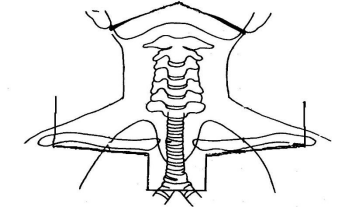
Figure 7 Standard irradiation fields for routine irradiation of thyroid cancer
C. Hybrid X-ray and electron irradiation technique (Figure 9): first high-energy X-ray front-to-back large field irradiation or single anterior field X-ray irradiation, 3 cm of lead blocking in the center of the anterior neck at DT 36-40Gy to continue X-ray irradiation, while the lead blocking part is irradiated with electron rays of appropriate energy, which ensures sufficient dose to the target area and keeps the exposure to the spinal cord within the safe dose range.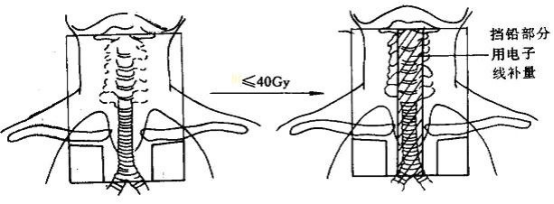
Figure 9 Hybrid high-energy X-ray and electron ray irradiation technique
The dose reference point is chosen around the anterior border of the cervical vertebrae. 40Gy of DT is still within the tolerated dose range for the spinal cord, and the thyroid, neck and upper mediastinum can be satisfactorily distributed. In the final dose increase, the lower border was moved up to the level of the thoracic notch and replaced by bilateral horizontal field pairs or two anterior oblique field wedges to achieve a total radical dose.
Fig. 10 Dose distribution of the small bucket field irradiation technique (10 MV X-rays)
3) Radiation source: Cobalt-60 or 4-6MV high-energy X-rays, 8-15 MeV electron rays.
4) Irradiation dose: slightly different according to the radiotherapy protocol (large split protocol and conventional split radiotherapy protocol). According to the conventional dose fractionation: fractionated dose of 200 cGy once a day, 5 times a week, 5000 cGy in large field, then increase the dose to 6000-7000 cGy for the residual area in the reduced field, and pay attention to the spinal cord not to exceed the tolerated amount. Foreign treatment guidelines recommend 70 Gy for lesions with visual residual, 66 Gy for microscopic residual or surgically removed tumors, 60 Gy for residual high-risk microscopic lesions (including the thyroid bed, tracheoesophageal sulcus, and lymph node drainage area in region VI), and 54-56 Gy for low-risk microscopic lesions (including uninvaded regions III-V and upper mediastinal lymph nodes).
- Complications of EBRT
(1) Acute complications: 1 to 2 degree reactions are more common, about above, including pharyngitis, mucositis, dry mouth, taste changes, dysphagia, painful swallowing, radiation dermatitis, etc. Above 3 degree reactions are rare, with the highest incidence of pharyngitis (<10) and the rest of reactions .
(2) Long-term complications: including skin muscle fibrosis, esophageal tracheal stenosis, pharyngeal stenosis leading to dysphagia, internal carotid artery sclerosis, and second primary cancer.