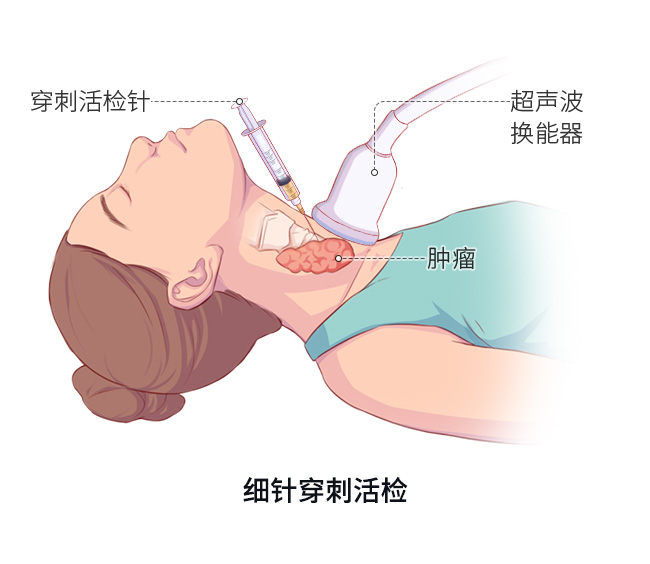
What is a fine needle aspiration biopsy?
Fine-needle aspiration (FNA) is a procedure in which a thin needle is inserted into a thyroid nodule and some of the cells are extracted and sent for examination. The pathologist looks at the cells under a microscope and identifies whether they are benign or malignant. Ultrasound guidance is also usually required for more accurate puncture localization.
FNA is simple, less invasive, has fewer complications, and has high safety and diagnostic accuracy; however, the amount of cells obtained is relatively small, and there is a risk of “false negatives” (failure to obtain tumor cells).
Why do I need a puncture biopsy when I’ve already had an ultrasound?
Ultrasound is the test of choice for thyroid nodules and is often used for the initial differential diagnosis. The ultrasound alone is difficult to “characterize” because thyroid cancer is insidious and the early signs and symptoms are similar to those of a benign nodule; the ultrasound can only identify benign and malignant nodules based on their “appearance” and relies on the physician’s experience. In order to find stronger evidence, a fine needle aspiration biopsy is needed to obtain a more accurate diagnosis by cell morphology.
The American Thyroid Association (ATA) considers FNA to be the most accurate and cost-effective method for diagnosing thyroid nodules, and it has been adopted as the gold standard for the initial diagnosis of benign and malignant thyroid nodules.
Puncture biopsies suggesting thyroid cancer are more than 95% compatible with postoperative pathology, so surgery should be performed as soon as possible; if the puncture is “negative” (no sign of malignancy), unnecessary surgery may be avoided.
You should be aware that there is a risk of “false negatives” in the diagnosis of thyroid cancer by fine needle aspiration: a “negative” aspiration result is actually a malignant tumor. The percentage is about 2% to 18%. This test alone may result in a “missed diagnosis”. In addition, due to the current state of medical technology, about 10% of patients are not diagnosed.
In summary, doctors recommend that if a checkup reveals a suspicious thyroid nodule and you are wondering whether to have surgery, you may want to start with a fine needle aspiration. Even if the report suggests benign, regular follow-up should continue.
When is an FNA needed?
- There is a basic clinical certainty of malignancy that requires fine needle aspiration to define the type of pathology. For example, if there is elevated calcitonin, it may be medullary thyroid cancer; if the tumor is progressing very rapidly, it may be undifferentiated cancer. The pathogenesis and treatment strategy of different pathological types of tumors are different, and preoperative puncture to clarify the pathological type can help the surgeon make better preoperative preparations
- Ultrasound examination suggests suspicious malignant nodes. The higher the grade, the greater the risk of malignancy. grade 4 is considered suspicious for malignancy, and usually an ultrasound grade of 4A or 4B is recommended for puncture; grade 4C or even 5 is usually recommended for direct surgery.
- Recent hoarseness, rapid increase in nodule size, and suspicious enlarged lymph nodes in the neck. These symptoms also suggest a greater likelihood of malignancy, and puncture is recommended.
If you want to know more about what the TI-RADS grading system means, please read the related article:
Which patients do not need FNA?
Puncture is generally not recommended for some low-risk nodes, such as those with a B ultrasound TI-RADS grade of 3 or less, or nodes that are 5 mm or less in size.
Which patients should not have an FNA?
Fine needle aspiration is generally safe, but your doctor may not recommend it in patients with the following risk factors:
- With a bleeding tendency (e.g., low platelet count, prolonged clotting time, history of unexplained bleeding, etc.), you may want to wait until you have corrected the clotting problem before performing the puncture.
- The nodule may be a hemangioma. Uncontrolled bleeding may occur with a puncture.
.
Summary
Fine needle aspiration biopsy, which is currently the most reliable method for preoperative diagnosis of benign and malignant thyroid nodules, is not necessary in all patients with thyroid nodules. Doctors usually recommend this test to confirm the diagnosis in patients with clinical or ultrasound suspicion of malignancy. Please follow your doctor’s instructions.
Related reading:
Co-written by Dr. Yiming Cao, Fudan University Cancer Hospital