1. What are bone marrow and hematopoietic stem cells?
.
Bone marrow is a soft, spongy substance that exists inside the bones. Bone marrow contains immature cells, such as hematopoietic stem cells or blood-forming stem cells. Unlike the familiar embryonic stem cells, which can develop into a variety of different types of somatic cells, hematopoietic stem cells can divide and form more hematopoietic stem cells, or mature blood cells, including infection-fighting white blood cells, red blood cells that carry oxygen, and platelets that have clotting functions.

Most hematopoietic stem cells are found in the bone marrow, but some are also present in the bloodstream after mobilization by certain drugs, called peripheral blood stem cells (PBSCs). In addition, the umbilical cord blood of infants also contains PBSCs. Hematopoietic stem cells from either source can be used for transplantation.
2. What are bone marrow transplantation and peripheral blood stem cell transplantation?
Bone marrow transplantation (BMT) and peripheral blood stem cell transplantation (PBSCT) are processes in which stem cells are destroyed by high-dose chemotherapy and/or radiation therapy and then reconstituted through transplantation. The process of PBSCT is the destruction of stem cells in the body by high-dose chemotherapy and/or radiation therapy, followed by the reconstruction of stem cells through transplantation.
There are three main types of transplantation:
- Autologous transplants: using the patient’s own stem cells for transplantation.
- Syngeneic transplants: Using stem cells from the patient’s identical twin for transplantation.
- Allogeneic transplants: Using stem cells derived from the patient’s sibling or parent for transplantation. Transplantation can also be performed using stem cells from a person who is not related by blood.
.
.
.
3. Why use bone marrow transplantation and peripheral blood stem cell transplantation to treat cancer?
First, patients are treated with very high doses of chemotherapy and/or radiation therapy before bone marrow transplantation or peripheral blood stem cell transplantation. To understand why stem cell transplantation is used for treatment, one needs to understand the antitumor effects of chemotherapy and radiation therapy.
Chemotherapy and radiation are usually effective against cells that divide rapidly, and tumor cells usually divide more rapidly than normal cells, so using chemotherapy or radiation can control tumor progression. However, because bone marrow cells also divide rapidly, high doses of antitumor therapy usually severely damage the patient’s bone marrow, resulting in bone marrow suppression. Without a healthy bone marrow, the patient’s body will not be able to produce red blood cells for carrying oxygen, white blood cells for fighting infection, and platelets for clotting, a consequence that can be fatal.
And after stem cells are destroyed, timely replenishment of the body with healthy stem cells through bone marrow transplantation or peripheral blood stem cell transplantation can restore the bone marrow’s ability to produce blood.
In addition, in some types of leukemia, the graft-versus-tumor (GVT) response that occurs after allogeneic hematopoietic stem cell transplantation is critical to ensure the effectiveness of the transplant. This is because the donor’s leukocytes recognize the cancer cells remaining in the patient’s body and thus attack them.
4. What cancers can be treated with bone marrow transplantation and peripheral blood stem cell transplantation?
.
Bone marrow transplantation and peripheral blood stem cell transplantation are most commonly used to treat leukemia and lymphoma. Transplantation works best when the leukemia or lymphoma is in remission (i.e., signs and symptoms are gone).
In addition, it is also used to treat other cancers, such as
- Neuroblastoma: A tumor that arises from immature nerve cells, most often seen in infants and children.
- Multiple myeloma.
Some clinical studies have also attempted to use hematopoietic stem cell transplantation for the treatment of other different tumors.
5. How do you find a suitable matched donor in allogeneic or allogeneic allogeneic transplantation?
.
To minimize potential side effects, doctors often want the donor’s stem cells to match the patient’s own stem cells as closely as possible. But different people have different sets of proteins on the surface of their stem cells, called “human leukocyte-associated antigens” (HLA antigens), which are called “HLA typing” and can be identified by a special blood test.
In most cases, the success of an allogeneic transplant depends on how well the donor matches the patient’s stem cell HLA typing. The higher the number of matched HLA antigens, the higher the success rate of the transplant and the lower the likelihood of post-transplant complications of “graft-versus-host disease”.
People who are more closely related, especially siblings, are more likely to be a match for the patient’s HLA than those who are unrelated. However, only 25% to 35% of patients have HLA-matched siblings, and the odds of obtaining HLA-matched stem cells from an unrelated donor are somewhat higher, at about 50%. The likelihood of HLA-matched siblings is even higher in the same race and ethnicity. Despite the current overall increase in the number of donors, there are still some patients who have difficulty finding a suitably matched donor.
Because identical twins have the same genes, their HLA antigens are the same and there is no question of a match, yet the odds of identical twins in the population are very low and therefore examples of homozygous transplantation are rare.
6. How are bone marrow stem cells collected for transplantation?
.
The stem cells used in a bone marrow transplant come from the bone marrow. The process of obtaining bone marrow is called “harvesting,” and the three types of bone marrow transplants-autologous, allogeneic, and allogeneic-are similar in the way they are harvested:
- Donors can be given general anesthesia, which is performed in a sleep-like state, or local anesthesia for the lumbar spinal nerve, which causes unconsciousness and no pain below the waist.
- A needle is then inserted through the skin into the iliac bone or, rarely, into the sternum to extract the bone marrow.
The collection of bone marrow usually takes about an hour.
The collected bone marrow is processed and can then be preserved with preservatives and frozen until it is needed. This technique is called “cryopreservation,” and stem cells can be stored cryopreserved for many years.
7. How are peripheral blood stem cells collected for transplantation?
How are peripheral blood stem cells collected for transplantation?
The stem cells used in peripheral blood stem cell transplantation (PBSCT) come from the bloodstream and can be obtained through a technique called apheresis or leukapheresis.
4 to 5 days before the “blood cleanse,” the donor takes a drug to increase the number of stem cells released into the bloodstream.
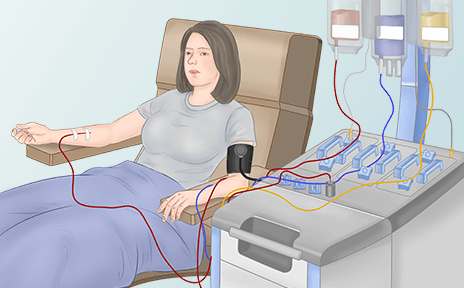
During the “cleanse,” blood is drawn through a large vein in the arm or a central vein (a flexible cannula inserted into a large vein in the neck, chest, or groin), and the blood is passed through a machine that separates the stem cells before being returned to the donor. The collected stem cells are then preserved.
The “clearing” process usually takes 4 to 6 hours. The stem cells are frozen and stored until they are needed.
8.
8. How are the cord blood stem cells collected?
.
For a cord blood transplant, the mother must contact a cord blood bank before the baby is born. After the baby is born, the umbilical cord is cut and the doctor collects blood from the cord and placenta.
If the mother agrees, the cord blood can be processed and frozen for preservation by the cord blood bank. However, the umbilical cord and placenta can only provide a small amount of blood, so the stem cells are collected and usually used only in children.
9. Is it dangerous to donate bone marrow?
.
Because only a small amount of bone marrow is removed during a bone marrow donation, there is usually no risk to the donor’s health. The risk comes mainly from anesthesia.
After donating bone marrow, the body part from which the marrow was taken may feel stiff or sore and tired for a few days. After a few weeks, the donor’s bone marrow is able to regenerate and recover. However, the time it takes to recover varies from person to person, with some people returning to normal in 2 to 3 days and others taking up to 3 to 4 weeks to fully recover.
10. Is it dangerous to donate peripheral blood stem cells?
.
During peripheral blood stem cell donation, “apheresis” (blood cleansing) usually causes mild discomfort, and donors may experience dizziness, cold shivers, numbness in the lips, and cramps in the hands. Unlike bone marrow donations, peripheral blood stem cell donations do not require anesthesia. However, a drug is applied to stimulate the bone marrow to produce stem cells and release them into the bloodstream, known as “stem cell mobilization,” a process that may cause skeletal muscle pain, headache, fatigue, nausea, vomiting, insomnia, etc. These side effects usually disappear 2 to 3 days after the last dose.
11. What happens after the stem cells are transplanted into the patient?
.
After receiving high-dose chemotherapy and/or radiation therapy, the patient undergoes a stem cell transplant by intravenous infusion, similar to a blood transfusion. This procedure usually takes 1 to 5 hours.
When the stem cells enter the patient’s circulation, they reach the bone marrow, where they produce new white blood cells, red blood cells, and platelets. This process usually occurs 2 to 4 weeks after transplantation, and doctors monitor blood counts regularly. However, full recovery of immune function takes longer, about several months for autologous transplant patients and 1 to 2 years for allogeneic or syngeneic transplant patients. Doctors perform various blood tests to make sure that new blood cells are being produced and that the tumor has not returned. Bone marrow aspiration tests can also help doctors determine if the bone marrow is recovering well.
12.
12. What are the side effects of bone marrow transplantation and peripheral blood stem cell transplantation?
.
The biggest risk of either bone marrow transplant or peripheral blood stem cell transplant comes from an increased risk of infection and bleeding from high-dose chemotherapy and radiation therapy. Doctors will give patients antibiotics to prevent infection. Patients may also be given platelet transfusions to prevent bleeding, or red blood cell transfusions to treat anemia. In addition, patients who receive a bone marrow transplant or peripheral blood stem cell transplant may experience some transient adverse reactions, such as vomiting, nausea, fatigue, loss of appetite, mouth ulcers, hair loss, and skin reactions.
Some potential long-term risks include some complications from pre-transplant chemotherapy and radiation therapy, such as infertility, cataracts, secondary tumors, and liver, kidney, lung, and heart damage.
Allogeneic transplantation may cause graft-versus-host disease (GVHD), which causes skin, liver, and intestinal damage. It can occur within a few weeks after transplantation (acute GVHD) or long after transplantation (chronic GVHD). To prevent this complication, patients need to take immunosuppressive drugs. In addition, the donor’s stem cells can also be treated to remove the white blood cells that may trigger GVHD.
Once GVHD occurs, it is often severe enough to require hormonal and immunosuppressive drug therapy.GVHD is difficult to treat, but some studies suggest that patients with leukemia who develop GVHD rarely have cancer recurrence. Some clinical trials are currently investigating how to prevent and treat GVHD.
13. What is a “micrograft”?
Micrografting (mini-transplantation)
Micro-transplantation, also known as non-cleared marrow transplantation or reduced intensity transplantation, is a type of allogeneic transplantation. It is currently in clinical trials for the treatment of many different types of cancer, including leukemia, lymphoma, multiple myeloma, and other hematologic tumors.
Microtransplantation uses lower-dose, less toxic chemotherapy and/or radiation regimens for pre-transplantation. This lower-dose antitumor therapy can eliminate some, but not all, of the bone marrow stem cells. It is also able to reduce the number of cancer cells and suppress the immune system to prevent transplant rejection.
Unlike traditional bone marrow transplantation and peripheral blood stem cell transplantation, both donor and patient stem cells are present in the patient’s body for a period of time after microtransplantation. Once the donor-derived stem cells begin to implant in the bone marrow, they may develop a graft-versus-tumor (GVT) effect and begin to destroy cancer cells that were not eliminated during pretreatment with radiation or chemotherapy. To enhance the GVT effect, the doctor may inject the patient with donor white blood cells. This process is called “donor lymphocyte infusion.
14.
14. What is a “secondary transplant”?
The second transplant (tandem) is a form of lymphocyte infusion.
Tandem transplant is a type of autologous stem cell transplant. It is in the clinical research phase and is used to treat a variety of tumors, including multiple myeloma and germ cell tumors. In a secondary transplant, the patient receives two successive high-dose chemotherapy treatments plus stem cell transplantation. Usually, the two procedures are several weeks to months apart. The researchers hope that this approach will stop the tumors from coming back.