What is cervical lymph node dissection?
Clinically, 30% to 80% of patients with thyroid cancer already have metastatic lymph nodes in the neck at the time of diagnosis (Table 1). In addition to removal of the thyroid gland, they need to undergo “cervical lymph node dissection,” which is a complete removal of the lymphatic tissue and surrounding fat, muscle, nerves, and blood vessels in the neck to destroy the metastases and reduce the risk of recurrence.
| Table 1. Incidence of cervical lymph node metastasis in thyroid cancer | |
| Percentage of metastases | |
| Papillary carcinoma | 30% to 60% |
| Follicular carcinoma | 10% to 20% |
| Medullary carcinoma | 30% to 50% |
| Undifferentiated carcinoma | 60% |
For differentiated thyroid cancer, radical thyroidectomy, which includes a two-step approach of thyroidectomy and cervical lymph node dissection, is currently recognized as the preferred and best treatment.

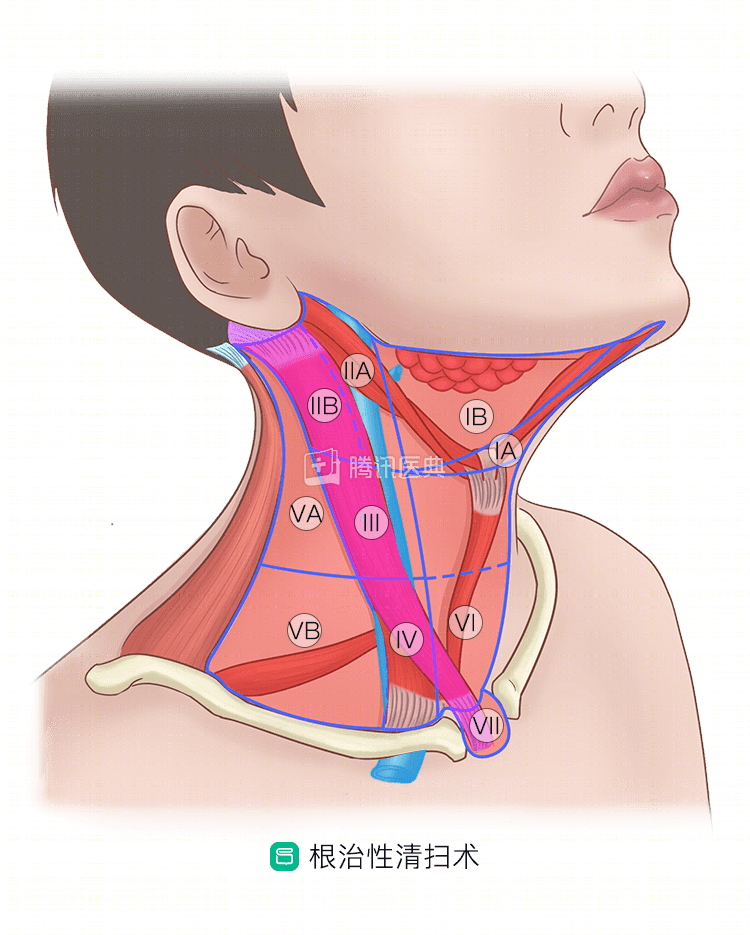
Figure Note: Internationally, cervical lymph nodes are divided into 7 zones, identified by Roman numerals I to VII. The lymph nodes in zones VI-VII are the central zone lymph nodes, and zones I-V are the lateral cervical zone lymph nodes. The lymph node metastasis of thyroid cancer is most common in the central region, followed by the lateral cervical region.
Why do we need to do a cleanse?
Like other tumors, thyroid cancer cells tend to metastasize through the lymphatics, and the lymph nodes along the way become a staging area and shelter for the cancer cells. The central cervical lymph nodes are often the first stop for metastasis, which may then metastasize to the lateral neck, and to lymph nodes farther away. At this point, even if all of the glandular tissue is removed, the cancer cells in the lymph nodes have already planted the seeds of metastasis and recurrence.
The goal of lymph node dissection is to completely remove the sentinel sites where cancer cells may be lurking.
What conditions require debulking?
- Lymph nodes in the central region
Even in relatively early-stage thyroid cancer, the risk of central zone lymph node metastasis is high, and even in some patients (about 30%), no lymph node metastasis is found on preoperative or intraoperative examination, but metastasis is found on postoperative pathology. Therefore, national experts prefer, regardless of whether lymph node metastasis is suspected on preoperative examination or during surgery, to do an ipsilateral central zone lymph node dissection once intraoperative frozen pathology confirms thyroid cancer.
The current concept abroad is different, and central zone lymph node dissection is done only in patients with preoperative confirmation of possible lymph node metastasis, or locally advanced disease.
- Lateral cervical zone lymph nodes
Lateral cervical zone lymph node metastases occur relatively infrequently and are relatively invasive, and it is now accepted that lymph node dissection should be performed only if there is a high suspicion of, or confirmation of, lateral cervical zone lymph node metastases on preoperative examination.
What types of debulking are available?
There are several different types of lymph node dissection in the neck.
- Radical dissection
This was the earliest procedure performed, and involves sweeping the entire cervical lymph nodes while removing the ipsilateral sternocleidomastoid muscle, internal jugular vein, and collateral nerves, preserving the common carotid artery, vagus nerve, and sympathetic nerve (below). It is now gradually being replaced by functional sweeping.
- Functional Clearing
Clearance of the entire cervical lymph nodes but preservation of the sternocleidomastoid muscle, internal jugular vein, and spinal paraspinal nerve, or portions thereof (below).

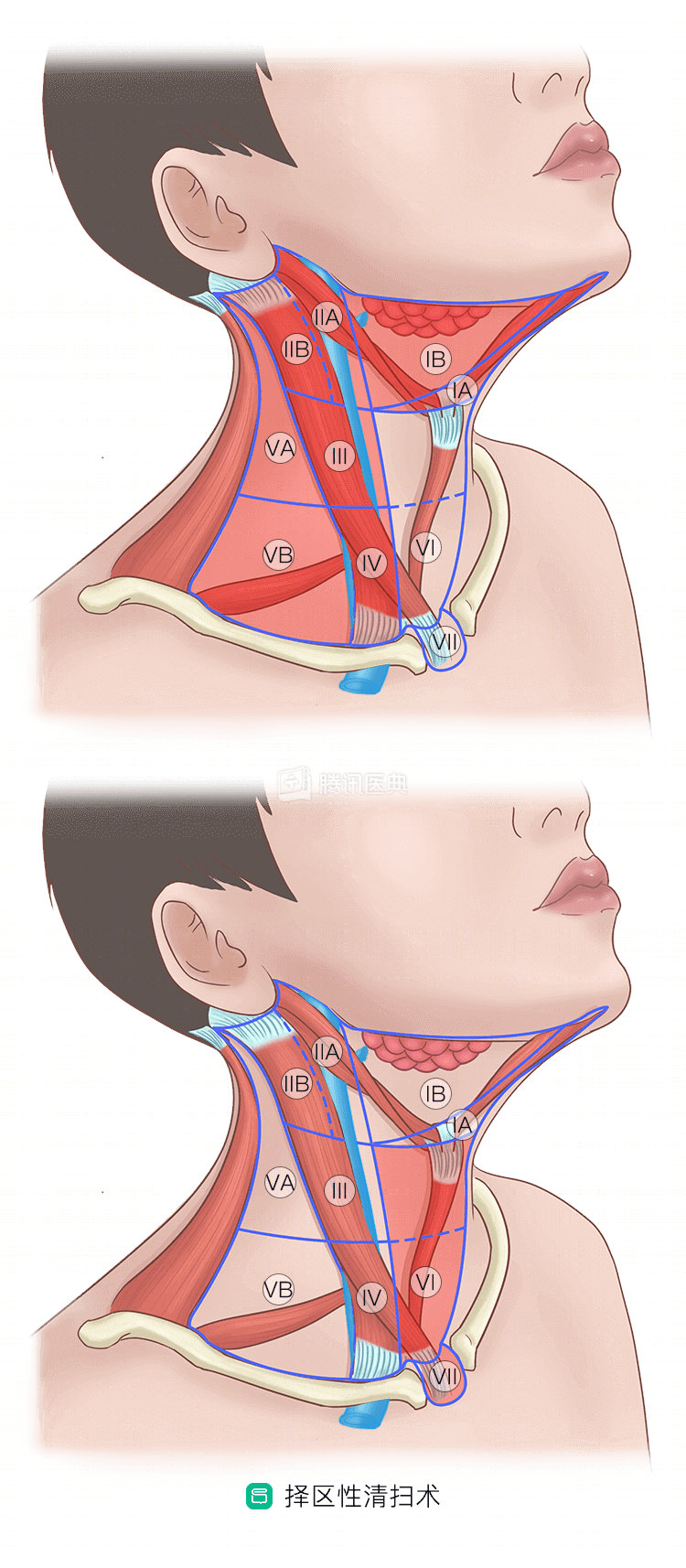
- Selective Zone Clearance
Selective debulking of lymph nodes in one region, such as the central or lateral cervical region.
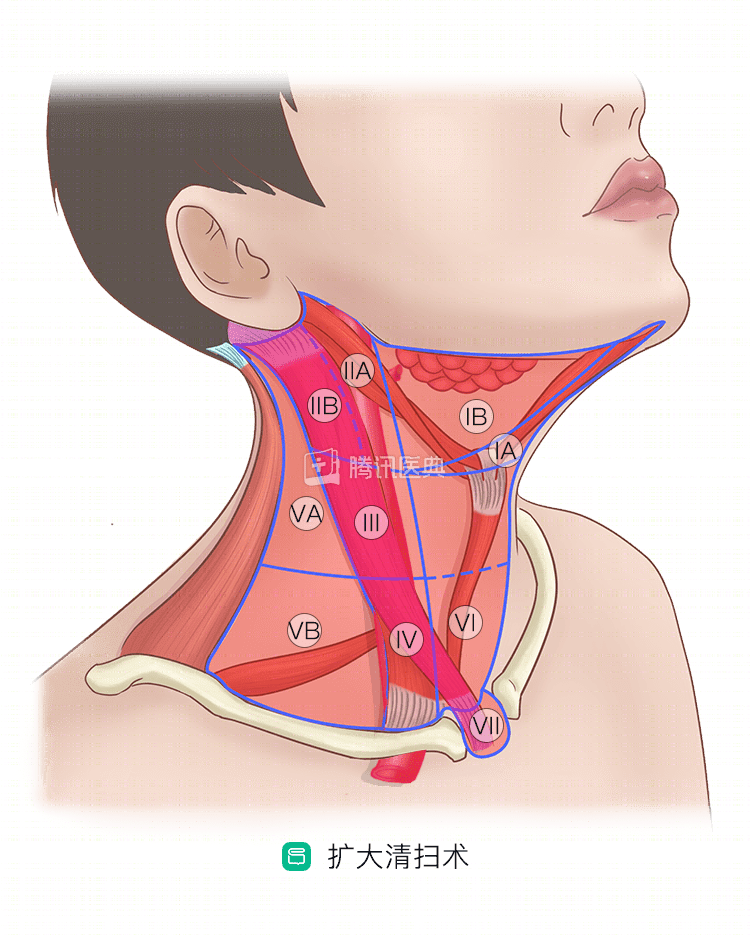
- Enlarged dissection
If there is significant extravasation of metastatic lymph nodes, invasion of internal jugular vein, sternocleidomastoid muscle, etc., an expanded clearance is required. The lymph nodes in zones I-V, or zones VI and VII, are cleared, and the tumor-invaded tissues, including the common carotid artery, vagus nerve, and phrenic nerve, are removed.
Currently, most thyroid cancers are treated with elective central zone clearance, or functional lateral neck clearance.
Co-written by Dr. Tingting Zhang, Cancer Hospital, Fudan University