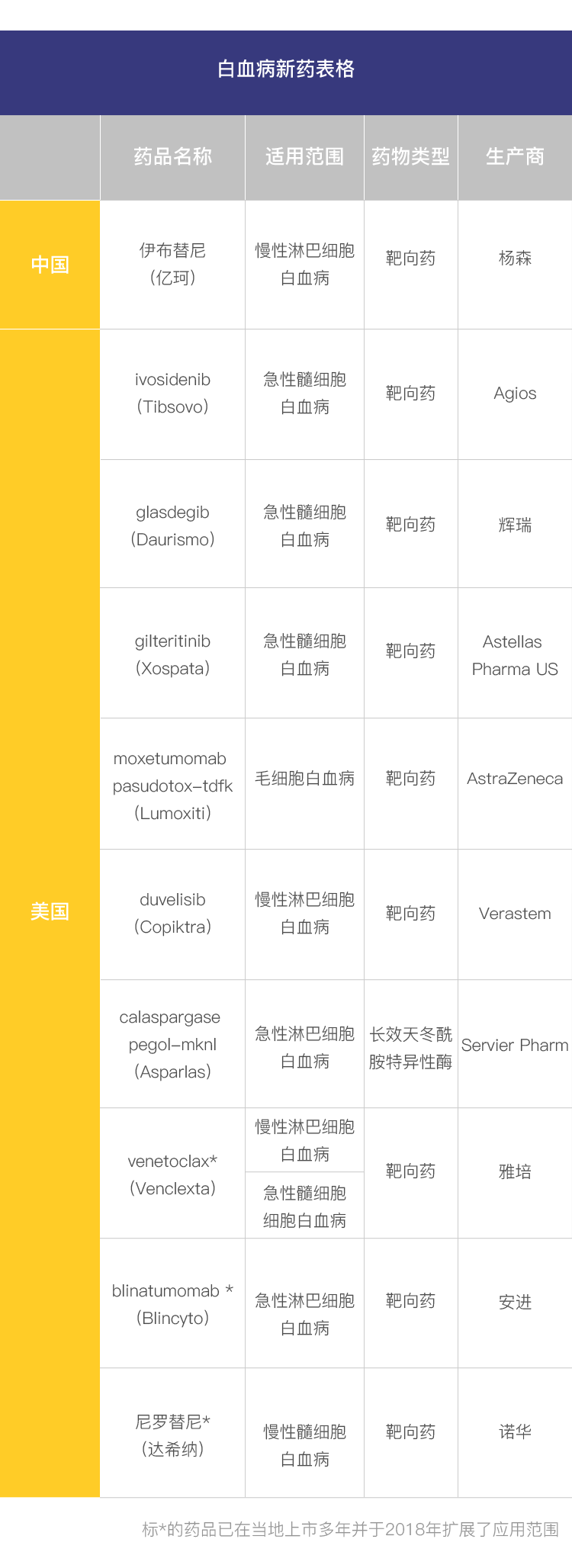
In 2018, ibrutinib was approved for marketing in China, and a total of six new leukemia drugs were approved for marketing in the United States, and three marketed drugs were expanded. They are listed below:
How do these new drugs work? For what kind of patients? We invited Professor Ma Jun from the Harbin Institute of Hematology and Oncology, a leading expert in the field, to give you an analysis.
What patients are the new drugs for?
Acute myeloid leukemia: glasdegib, venetoclax, gilteritinib, and ivosidenib
80% of patients with acute leukemia have acute myeloid leukemia, a rapidly progressive cancer in which less than a quarter of patients survive longer than 5 years. Initial treatment is now primarily with chemotherapy, but older patients (over 75 years of age) often cannot tolerate the side effects of chemotherapy. glasdegib and venetoclax, new drugs coming to market in 2018, are targeted at this group of patients.
Glasdegib is a targeted drug that inhibits the Hedgehog signaling pathway, a pathway associated with rapid cancer cell growth. In the study, glasdegib combined with initial treatment with cytarabine resulted in an overall survival (OS) time of 8.3 months for patients, twice as long as the previous standard treatment.
And venetoclax is a BCL2 inhibitor. bcl2 is caused by a deletion of chromosome 17 and is associated with rapid cancer progression. In patients over 75 years of age, venetoclax combined with low-dose cytarabine led to remission in 70% of patients.
Regardless of age, once initial treatment fails and the disease recurs, there is almost no cure. The two new drugs that “entered” the market in 2018, gilteritinib and ivosidenib, are aimed at patients with relapses.
Gilteritinib is an orally targeted agent that inhibits FLT3 mutations. Previous studies have found that about 25% to 30% of patients with acute myeloid leukemia carry FLT3 mutations, and these patients are more likely to relapse. in 2017, the drug quizartinib, which targets FLT3, was approved for marketing in the U.S. in 2018, the comparable drug gilteritinib was approved for marketing, and it led to remission in 22% of patients in the study. the FDA requires that, before genetic testing before using the drug, and only the clear presence of FLT3 mutations should be treated with gilteritinib.
Ivosidenib is also a targeted agent that inhibits IDH1 mutations. This type of mutation has also been associated with cancer recurrence. In the study, it led to complete remission in 32.8% of patients. Genetic testing is also needed before using the drug, and it should only be used if the IDH1 mutation is clearly present.
Chronic myeloid leukemia: nilotinib
Nilotinib, approved in 2018, is primarily for children with chronic myeloid leukemia. Chronic myeloid leukemia accounts for less than 3% of all children with leukemia, but children typically progress more rapidly and have limited treatment options compared with adult patients. And because of the small number of patients with the disease, there are usually fewer clinical trials, further limiting treatment options for such children.
Nilotinib is a drug that targets the Philadelphia chromosome mutation, a class of drugs that includes the big name “Gleevec”. Studies have shown that in children aged 2 to 18 years, remission rates at the molecular level are over 60% after 12 cycles of nilotinib and over 40% after 12 cycles even as second-line therapy; both are significantly better than current therapy.
Acute lymphoblastic leukemia: calaspargase pegol-mknl and blinatumomab
Acute lymphoblastic leukemia is a rapidly progressive cancer. It is currently treated primarily with multidrug combination chemotherapy. Asparaginase is one of the components of the regimen. calaspargase pegol-mknl, approved in 2018, is a long-acting asparaginase that extends the dosing interval for patients.
While many patients respond well to chemotherapy, they often relapse. One of the main reasons for relapse is that cancer cells remain in the patient’s bone marrow during or after treatment, which is called “microscopic residual disease (MRD). The targeted drug blinatumomab minimizes the risk of recurrence by removing MRD. Studies have shown that it makes MRD undetectable in 85% of patients.
Chronic lymphocytic leukemia: duvelisib, venetoclax, and ibrutinib
Chronic lymphocytic leukemia and small cell lymphoma are actually different manifestations of the same disease. For patients with relapses of this leukemia, 3 targeted agents – duvelisib, venetoclax, and ibrutinib – were added in 2018.
In the study, duvelisib and ibrutinib had single-agent remission rates of 74% and 89%, respectively, while venetoclax combined with rituximab led to remission in more than 90% of patients. Moreover, all 3 drugs are oral and can be taken by patients at home, without the need for frequent hospital injections or hospitalization.
Hair cell leukemia: moxetumomab pasudotox-tdfk
Hairy cell leukemia is a rare, slow-growing leukemia caused by an excess of B cells (lymphocytes) in the bone marrow that look like “hair” under the microscope, hence the name hairy cell leukemia.
The new drug moxetumomab pasudotox-tdfk, which came on the market in 2018, is for hairy cell leukemia. It found that in adult patients who had relapsed or were refractory after receiving at least two systemic therapies, 30% achieved durable complete remission (CR) after treatment, with an overall remission rate (ORR) of 75%.
What is better about the new regimen?
In potentially curable patients, the goal of treatment is to maximize the chance of cure, so if 1 new regimen brings a higher rate of complete remission and time to remission, that means it is better than the previous regimen. The venetoclax, nilotinib, and others mentioned above have done well in this regard.
For leukemia with no hope of a cure, the goal of treatment is to control the disease and prolong progression-free survival as long as possible, and moxetumomab pasudotox-tdfk does this very well.
Is the new drug or regimen safe?
With these new drugs and regimens, one needs to be alert to their adverse effects. Among these drugs, glasdegib, ivosidenib, nilotinib, duvelisib, blinatumomab, and moxetumomab pasudotox-tdfk all have a “black box warning,” which is one of the most serious forms of warnings the FDA has ever placed on a marketed drug. This is one of the most serious forms of warning the FDA has ever given to a marketed drug, alerting that the drug may cause a lethal adverse reaction.
As a patient, don’t panic.
As a patient, it is important not to panic, but to discuss with an experienced medical professional to understand the adverse effects of the drug and to weigh the pros and cons of treatment options.
Can Chinese patients use these new regimens?
Can Chinese patients use these new regimens?
Most of these drugs are not available in China and are unlikely to be available to patients in China in the near future. However, these drugs do show efficacy in studies that are superior to traditional chemotherapy, and patients can access treatment by participating in clinical trials. At the same time, we hope that these new drugs will enter the country as soon as possible and benefit more patients with the help of the national policy on new anti-cancer drugs.
If you want to learn more about new drugs coming to market in 2018, please click to read