Differentiated thyroid cancer, which mainly includes papillary and follicular carcinomas, accounts for more than 90% of all thyroid cancers. This cancer is less malignant, and patients can have a 10-year survival rate of 85% to 95%.
Treatment is varied and includes surgery, radioiodine therapy, endocrine therapy, external radiation, and targeted therapy.
Surgical treatment
Surgery is the treatment of choice for thyroid cancer.
Surgery is the preferred treatment for thyroid cancer.
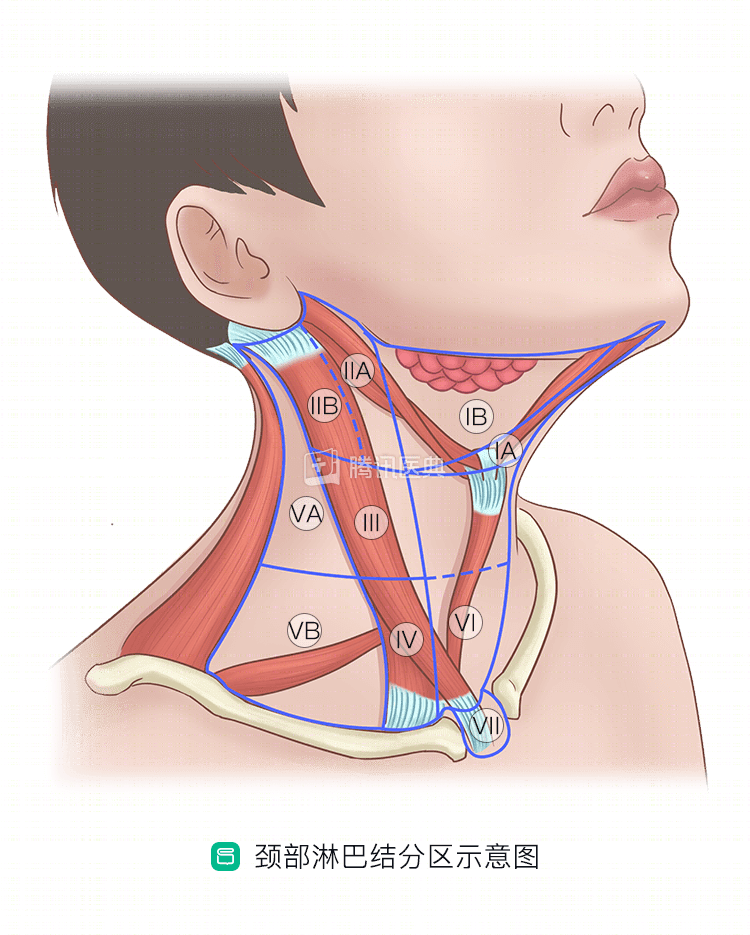
The ability to “cure” the patient with initial surgery is critical to the outcome. Depending on the stage of the tumor and the status of the lymph nodes, surgical options include lobectomy on one side of the gland + isthmus, total thyroidectomy/subtotal thyroidectomy, and lymph node dissection in the central zone (zone VI in the figure) / lateral neck area.
For locally advanced or recurrent thyroid cancer, the scope of surgery may involve adjacent organs, including the trachea, esophagus, and larynx.
Surgery is best performed in a specialized thyroid center or specialty group, by experienced specialists, and requires multidisciplinary collaboration including thoracic surgery, vascular surgery, plastic surgery, and intensive care unit (ICU) when necessary.
Studies have shown that there are recurrent lesions such as lymph nodes that are small in number and size, may not change over years of follow-up, and have not resulted in increased mortality. Therefore, physicians may also recommend follow-up for lymph nodes less than 0.8 cm in the central region and less than 1 cm in the lateral cervical region; if the lesion grows, surgical intervention is considered after re-penetration to confirm the diagnosis.
Related reading:
Radioactive iodine therapy (RAI)
The thyroid gland has a unique function – iodine uptake, so taking radioactive iodine (radioactive I-131), which is equivalent to radiation therapy inside the lesion, can kill thyroid cancer with precision. RAI therapy is extremely important for patients whose lesions cannot be completely removed by surgery, or who have developed lung or bone metastases.
Radioiodine therapy can be divided into “nail clearing” and “focal clearing” depending on the purpose.
“Clearing the nail”
Postoperative removal of microscopic lesions hidden in the residual thyroid tissue is called “nail clearing. For patients at high risk of recurrence, postoperative RAI therapy is now recommended to reduce recurrence and mortality.
Patients with a low risk of recurrence can transition directly to endocrine therapy (also known as TSH suppression therapy, which involves taking thyroxine tablets).
Related reading:
“Clear foci”
A metastatic thyroid cancer has developed, and treatment of the metastatic lesion with RAI is called “clearing”.
The effect of “clearing” is related to the following factors:
- The extent of iodine-131 uptake at the metastasis
- Duration of I-131 retention in the lesion
- Sensitivity of the lesion to I-131 radiation
- Age (younger patients are more likely to be cured)
- Size and location of metastases (smaller lesions in soft tissue and lungs are more likely to be cleared)
It is important to note that if the metastases have formed a large, substantial mass or if the bone metastases have caused bone destruction, even if the level of iodine-131 uptake is high, physicians will usually prioritize surgery followed by adjuvant RAI therapy.
In addition, in patients with local recurrence after surgery, lymph node metastases, and invasion of vital organs such as the trachea and esophagus, physicians usually also consider surgery first and then RAI therapy if residual disease remains after surgery.
Some patients have lesions that are not iodine-intolerant and have difficulty benefiting from RAI therapy, which is called “iodine-refractory thyroid cancer. These patients may now be considered for treatment with targeted agents such as sorafenib.
Endocrine therapy
Patients with differentiated thyroid cancer are generally treated with endocrine therapy, also called TSH suppression therapy, after surgery.TSH, known as thyrotropin, or thyroid stimulating hormone (TSH), is a hormone secreted by our pituitary gland that stimulates thyroid cell proliferation and hormone secretion when When thyroid hormone tablets [commonly used is levothyroxine sodium tablets (L-T4)] are taken to make the body’s thyroid hormone level higher, TSH secretion is reduced. This is the principle of TSH suppression therapy.
Usually blood TSH needs to be controlled at a level of 0.1 to 2 mU/L.
Related reading:
Targeted therapy
Targeted therapy is a new type of therapy that targets tumor-specific “targets” at the cellular molecular level.
There are currently four targeted drugs approved in the United States for the treatment of advanced thyroid cancer: sorafenib (Nexavar), lenvatinib (Lenvima), cabozantinib (Cometriq), and vandetanib (vandetanib). vandetanib (trade name caprelsa), of which sorafenib and levatinib can be used for advanced iodine-refractory differentiated thyroid cancer. Sorafenib has been marketed and entered into medical insurance in China, and several other drugs are in clinical trials in China and abroad.
It is important to note that according to US professional guidelines, targeted therapy is currently only used for advanced thyroid cancer that is progressing; it has not shown efficacy in patients with advanced but stable disease.
Related reading:
Summary
Surgery, radioiodine therapy, and endocrine therapy are common therapies for differentiated thyroid cancer, and patients with advanced disease who are not sensitive to these conventional treatments may consider the targeted agent sorafenib. The common “chemotherapy” and “radiotherapy (external radiation therapy)” used for other cancers are not effective for differentiated thyroid cancer and are usually not chosen.
Co-written by Dr. Jiaying Chen, Fudan University Cancer Hospital, and Dr. Weibo Xu