Leukemia cells can often invade the central nervous system, which is called central nervous system leukemia, CNSL, or “cerebral white”, with meningeal infiltration being more common.
Which leukemias are more likely to develop “cerebral white”?
Which leukemias are more likely to have “white brain”?
“Cerebral white” can occur in all stages of acute leukemia, both at the time of initial diagnosis and in remission.
- Patients with acute lymphoblastic leukemia (ALL) are more likely to have “white brain” than patients with acute myeloblastic leukemia (AML);
- Patients with childhood ALL are more likely to have “white brain” than adults with ALL.
- Patients with childhood ALL have a higher incidence of “white brain” than adults with ALL;
- Patients with T-cell ALL and Burkitt’s lymphoma/leukemia (formerly L3) are more likely to have “white brain”;
- Patients with acute myeloid leukemia are more likely to be M4 or M5 patients.
Why does “cerebral white” occur?
Why does “white brain” occur?
“Cerebral white” is mainly associated with a high tumor cell load at the time of initial diagnosis, such as a white blood cell count greater than 50×10/L at presentation, enlarged liver and spleen lymph nodes, and elevated lactate dehydrogenase levels.
The main routes of entry of leukemia cells into the CNS are: bloodstream dissemination, infiltration of cranial bone marrow leukemia cells, or intracranial hemorrhage.
Because of the presence of the blood-brain barrier, which prevents harmful substances from entering brain tissue, it is also difficult for general chemotherapy drugs to pass through, which does not effectively kill leukemia cells in the central nervous system, making the central nervous system a refuge for leukemia cells, leading to “brain whiteness” and becoming a cause of leukemia relapse.
What are the symptoms of “white brain”?
What are the symptoms of leukemia?
The symptoms and clinical manifestations of CNS leukemia depend on the site of infiltration, the size of the leukemic cells, and the number of sites involved.
Involvement of the brain
It can produce headache, altered confusion, abnormal walking, nausea, vomiting, coma, seizures, abnormal gait or sensation, optic papilledema, and abnormal blood pressure and heart rate; a small number of patients may have irritability, confusion, convulsions, and hemiparesis due to bleeding triggered by damaged and ruptured intracranial blood vessels, etc.
Involvement of cranial nerves
May lead to diplopia, impaired hearing and vision, numbness in the face, difficulty swallowing, and vertigo.
Involvement of the spinal cord
It can lead to loss of muscle strength in the limbs (especially the lower limbs), hemiplegia, back pain, radicular pain, bladder and bowel dysfunction.
How is “cerebral white” diagnosed?
Early detection and diagnosis
Early detection and diagnosis depends on close observation of these symptoms during the course of the disease, and once a patient is suspected of having CNS leukemia, appropriate tests should be performed as soon as possible to clarify. The main tests include radiology, cerebrospinal fluid cytology, and immunophenotyping by flow cytometry.
Magnetic resonance imaging, MRI
The preferred method of radiological examination.
Cranial nerve MRI enhancement or enlargement, soft meningeal nodule-like or linear enhancement into the sulcus or basal pool, and intradural enhancement nodules, especially changes in the cauda equina, are all suggestive of CNSL. MRI can also differentiate from white matter encephalopathy, cerebral atrophy, old hemorrhage, or infarct foci.
But MRI also has the problem of false positives or false negatives.
Cerebrospinal fluid examination
The most useful test for diagnosing CNSL.
Increased cerebrospinal fluid pressure, increased protein, decreased glucose, and increased white blood cell count are all suggestive of CNSL. Conventional cerebrospinal fluid cytology is highly specific for the diagnosis of CNSL, but is less sensitive and suffers from the same problem of false negatives.
Immunophenotyping by flow cytometry
The ability to detect 0.01% of leukemic cells is sensitive, but requires a high level of cerebrospinal fluid specimens: a sufficient amount of cerebrospinal fluid should be obtained at the time of lumbar puncture and sent for testing as soon as possible after obtaining the specimen, preferably within 1 h, to prevent destruction of leukemic cells from affecting the detection rate.
One study showed that patients with the presence of leukemic cells in the cerebrospinal fluid detected by flow cytometry had shorter relapse-free survival and shorter overall survival than patients with no leukemic cells detected.
Thus, screening for cerebrospinal fluid leukemic cell infiltration using flow cytometry immunophenotyping methods early in leukemia treatment should be performed in units where available to facilitate early diagnosis and early intervention.
Radiotherapy first? Or chemotherapy first?
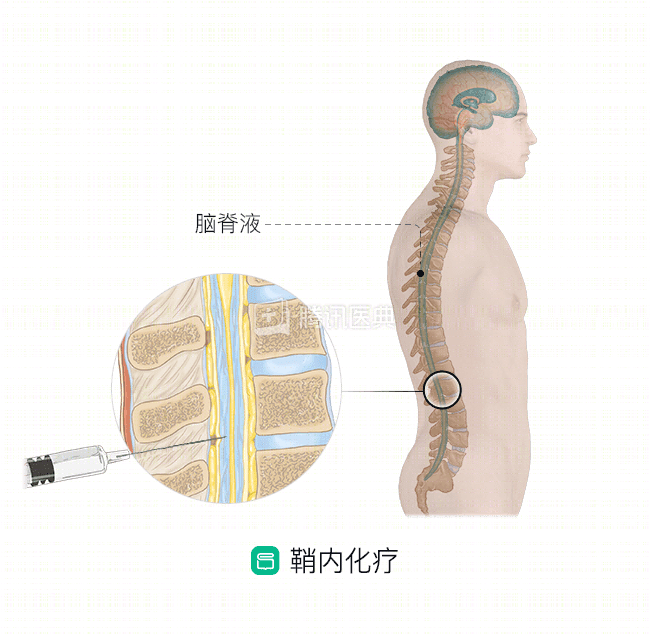
Once “cerebral white” occurs, lumbar puncture (lumbar puncture) and intrathecal chemotherapy should be administered as soon as possible to control the symptoms of “cerebral white.
Two lumbar punctures are usually performed weekly, and systemic high-dose chemotherapy should be administered at the same time, followed by radiation therapy after the clinical symptoms have resolved. Commonly used therapeutic agents include:
- Systemic administration: high-dose cytarabine, high-dose methotrexate, glucocorticoids
- Intrathecal administration: methotrexate, cytarabine, and glucocorticoids
- CAR-T immunotherapy: For patients with B-cell acute lymphoblastic leukemia, a CAR-T immunotherapy approach may be tried if the above treatment options are not effective.
It is important to note that lumbar puncture and sheath injection are in principle not performed six months after the end of radiotherapy.
Do you need a transplant?
Patients with “white brain” are high-risk patients and need to be considered for allogeneic HSCT, but after “white brain” occurs, lumbar puncture and intrathecal chemotherapy are needed to control the “white brain”. “The first step in the process of transplantation is the development of a new allogeneic hematopoietic stem cell transplant.