To understand what factors affect the success rate of hematopoietic stem cell transplantation, you first need to understand what types of hematopoietic stem cell transplantation are available.
Types of hematopoietic stem cell transplantation
- Homozygous hematopoietic stem cell transplantation: One of the identical twins is transplanted as a hematopoietic stem cell donor to the other, and because the genotypes are identical, it is called a homozygous transplant.
- Allogeneic HSCT: A transplant using another person’s (non-identical) healthy HSCs is called an allogeneic HSCT. If the donor is related to the patient, it is called a related donor transplant; if it is provided by a non-related donor, it is called an unrelated donor transplant.
- Umbilical cord blood hematopoietic stem cell transplantation: The umbilical cord blood of newborns is also rich in hematopoietic stem cells, and hematopoietic stem cell transplantation can be performed using the umbilical cord blood of newborns. However, because of the small number of HSCs it contains, cord blood transplantation is currently used more often in children. The collection of umbilical cord blood has no effect on the fetus or the mother, and is turning waste into treasure.
- Autologous hematopoietic stem cell transplantation: In an autologous transplant, the patient’s own normal hematopoietic stem cells are first collected and frozen, because chemotherapy and radiation therapy destroy a large number of normal hematopoietic stem cells along with the diseased cells in the body. Then, after high-dose radiotherapy, these cells are transfused back to the patient through the peripheral vasculature like a blood transfusion.
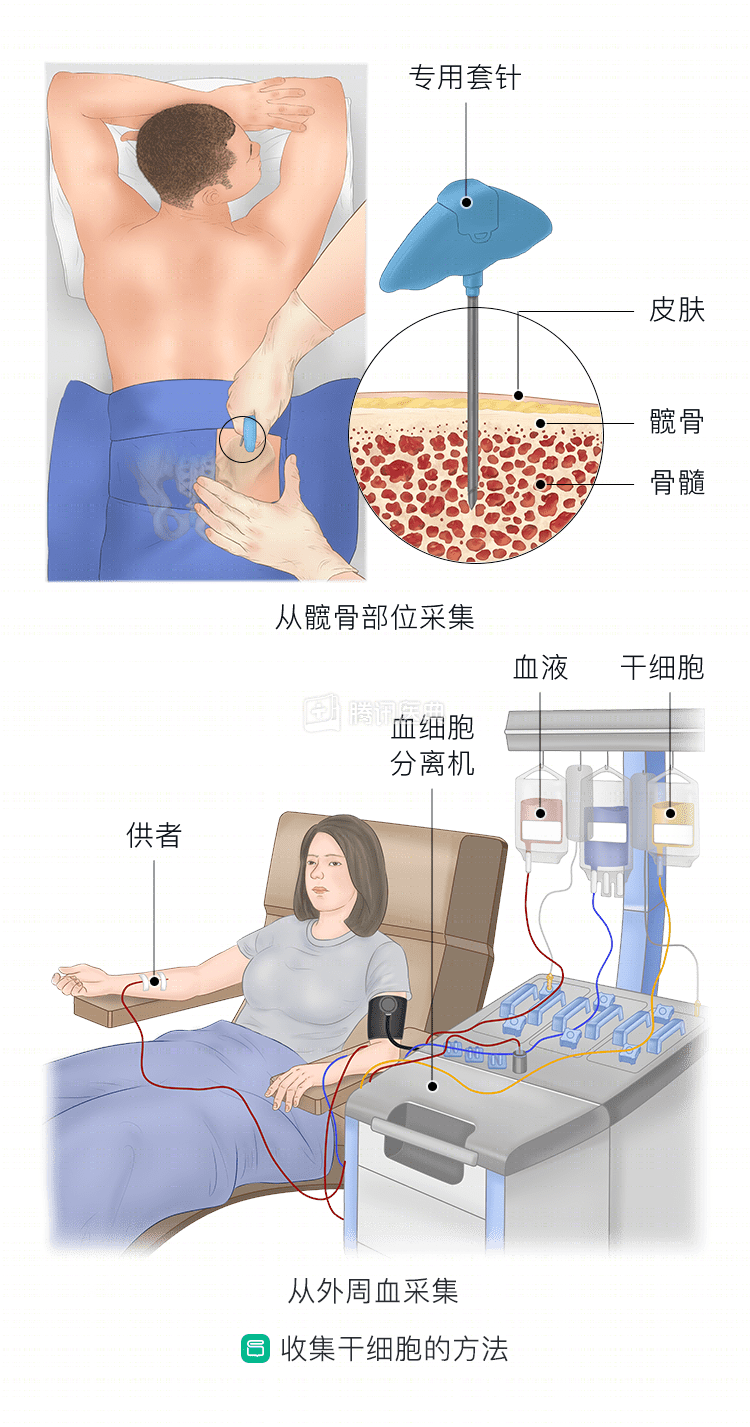
Key methods of collecting HSCs
Second, it is important to understand the main methods of collecting HSCs. There are two main methods, and the second one is mostly used today.
- Bone marrow HSC extraction: The donor is given general or local anesthesia and bone marrow blood is extracted from the bone marrow cavity of the donor’s pelvis.
- Hematopoietic stem cell collection from peripheral blood: The donor is given a subcutaneous injection of mobilizer and blood component mono-collection is performed using a blood cell separator to collect hematopoietic stem cells from the donor’s peripheral blood.
Focus on understanding the factors that affect the success of allogeneic HSCT
Allogeneic HSCT generally goes through four major hurdles: pre-transplant chemotherapy, transplantation, infection, and post-transplant rejection. Only when these four hurdles are successfully passed in turn, with regular tests related to microscopic residual lesions in the bone marrow, donor-recipient chimerism rate, and normal bone marrow, blood and vital organ tests, is the transplant truly successful.
The main causes of transplant failure are relapse, rejection, and infection. Some patients relapse after transplant discharge, which is related to the type of disease and disease status of the patient at the time of transplantation, organ function, autoimmune reaction, complications of the transplantation process and the matching rate of genetic loci between the donor and the patient, and the overall level of the transplantation hospital.
Several stages of the allogeneic HSCT process are critical to the success of transplantation:
- Pre-transplantation
- Pre-transplantation preparation: The type of disease and timing of transplantation before transplantation, such as allogeneic HSCT for acute leukemia, preferably in first complete remission or early relapse, and lymphoblastic lymphoma, preferably after first complete remission.
- Pre-treatment phase: Before HSCT, patients need to receive a course of high-dose chemotherapy and/or radiotherapy, during which the white blood cells also drop rapidly to almost 0. They need to be housed in a sterile laminar flow room, where the air is filtered to remove microorganisms and other particles before being imported, and those entering the clean room need to wear People entering the clean room need to wear sterile isolation clothes, hats, shoes, masks and gloves. Patients need to ensure daily cleanliness of the nasal, oral, perianal and other body skin.
- Donor stem cell mobilization and collection: Normally, peripheral blood contains a low percentage of hematopoietic stem cells; therefore, in order to collect a sufficient amount of hematopoietic stem cells, cytokines need to be applied to mobilize hematopoietic stem cells from the bone marrow into peripheral blood. On the fifth day after cytokine application, the peripheral blood hematopoietic stem progenitor cell level reaches its peak. The amount of hematopoietic stem cells mobilized and collected also directly affects the patient’s hematopoietic recovery and the success of transplantation
- Transplantation phase: Transfusion of hematopoietic stem cells from the donor back to the recipient through the vein is a process like a blood transfusion, but because some of the donors are not of the same blood type as the patient, even though as few red blood cells as possible have been collected during the stem cell collection process, a small number of red blood cells will inevitably remain, so some patients will have hemolytic reactions to blood type incompatibility, but most The stem cell transfusion can be safely completed after treatment.
- Early post-transplantation period: This is the period of time when the hematopoietic stem cells are implanted in the recipient and the blood cells recover to safer levels. This is the period when the patient is in myelosuppression and neutrophils, red blood cells, and platelets are at low levels, so this period also becomes an extreme period where the patient is prone to complications such as infections and bleeding, and aggressive prevention and treatment of infections and transfusion of blood products such as red blood cells and platelets can help the patient to pass through this dangerous period more safely.
- Mid-term post-transplantation period: After the donor’s hematopoietic stem cells have been implanted in the recipient, the recipient is under observation in the general ward. During this period, post-transplant complications are mainly observed or managed, and the recipient can be discharged if he/she is generally well and has no serious complications. Some patients may develop acute graft-versus-host disease (aGVHD), commonly known as “rejection reaction”, such as rash, diarrhea, jaundice, etc. Severe aGVHD may be fatal, therefore, active prevention and treatment of aGVHD is also the key to successful stem cell transplantation. Therefore, active prevention and treatment of aGVHD is also the key to successful stem cell transplantation.
- Later post-transplant period: Patients are discharged from the hospital with regular outpatient follow-up until about 6 months post-transplant, then return to the local area if they are stable, and are reviewed every 1-2 months until 2 years post-transplant, and then every 3 months until 5 years post-transplant. The main problems that may occur during this period are post-transplant relapse, chronic graft-versus-host disease, infection, etc. Early detection and early intervention can improve the success rate of transplantation. Regular post-transplant follow-up is one of the keys to ensure successful transplantation.