To cure leukemia, all leukemia cells, including stem cells, must be completely removed. How do we do it?
Currently, we know of 3 ways to treat leukemia: first, through hematopoietic stem cell transplantation; second, through targeted drug therapy; and third, immunotherapy. In fact, all three of these approaches have the potential to cure leukemia, which means that leukemia is not an “incurable” disease.
Hematopoietic stem cell transplantation
Hematopoietic stem cell transplantation works by taking normal human blood stem cells (usually either bone marrow or peripheral blood) and returning them to pretreatment patients (post-chemotherapy patients) so that the transfused cells can begin to rebuild blood and immune function in the body.
But the first prerequisite for HSCT is that “there must be a normal source of HSC,” or “donor,” as we call it. The traditional theory is that a 100% match between the donor and the recipient is necessary for a HSCT to be feasible. Such a small probability, even in China, seems to have failed to reverse the urgency of the situation, with only 11% of the approximately 2 million volunteer donors being a match.
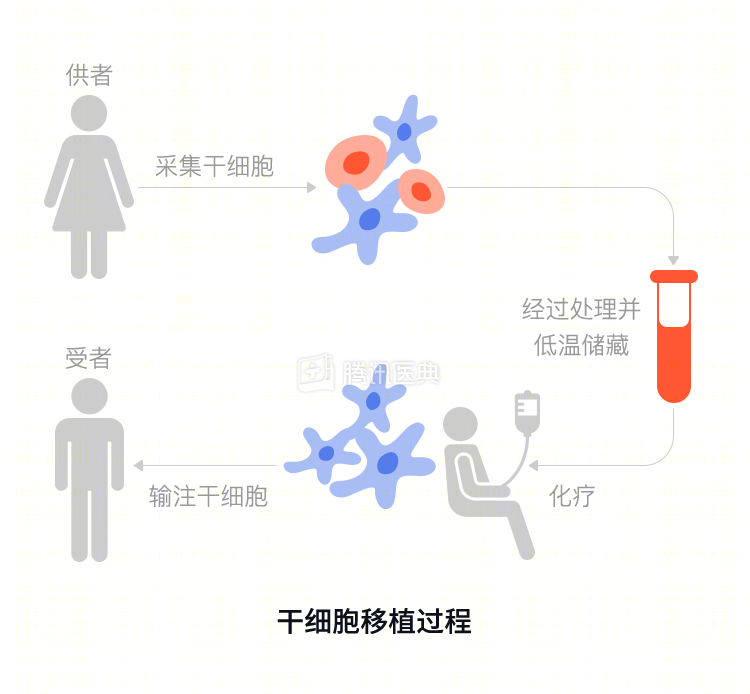
Is there a way to solve the donor source problem? The answer is yes. Haploidy, also known as “mismatch”, means that a 50% mismatch is sufficient, and the child and parents must be “haplotypes”. This makes haploidy a very good way to solve the problem of donor origin.
Targeted drugs
The second approach is to find specific markers on the surface of leukemic cells to kill. For example, in chronic granulocytic leukemia, a special chromosome was identified in 1960 from a patient with slow granulation in Philadelphia, USA, and to celebrate this major discovery, it was named the Philadelphia chromosome or Ph chromosome after the dump.
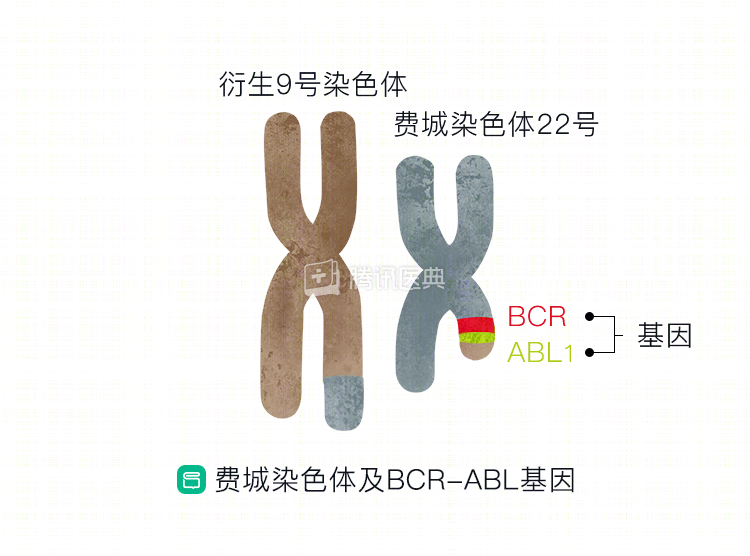
The Philadelphia chromosome refers to the translocation of chromosomes 9 and 22 in the human body, resulting in the oncoprotein p210. In 1994 Novartis invested heavily in the successful development of imatinib mesylate, an inhibitor of the p210 protein, which relegated hematopoietic stem cell transplantation therapy for patients with slow onset granulocytes to the second line.
Similarly, in acute promyelocytic leukemia, there is a chromosome 15 and 17 translocation that creates a PML/RARa fusion gene, which is the root cause of the disease. Retinoic acid binds to the RARa (retinoic acid receptor gene), not killing, but differentiating these cells into normal granulocytes (a mechanism that is even more bullish and original to China), so that acute promyelocytic leukemia can now be cured without transplantation.
Immunotherapy
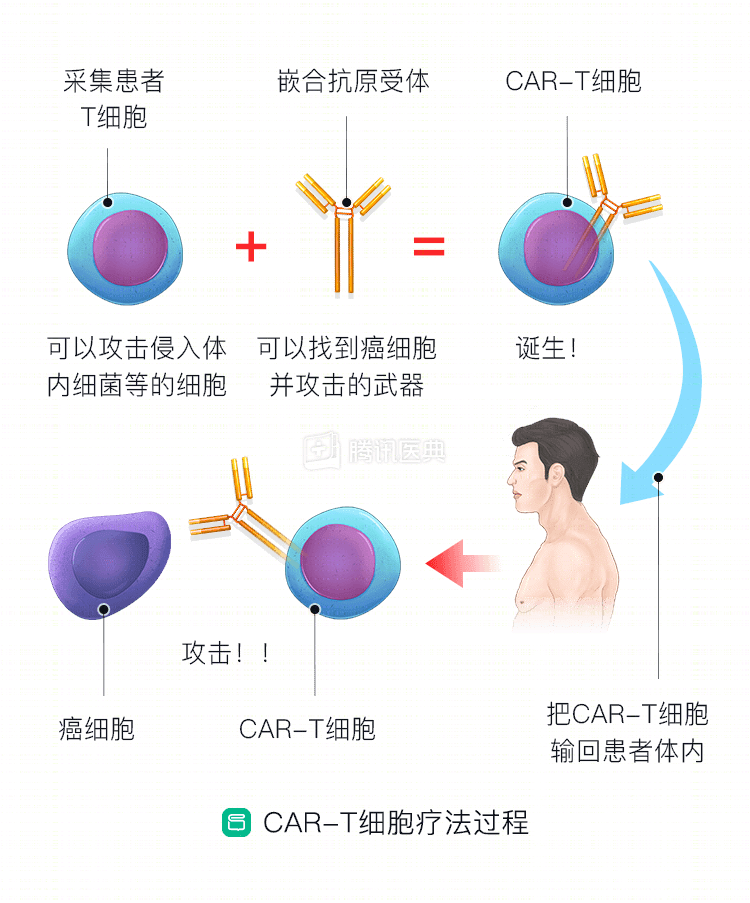
A third option is emerging: immunotherapy. Don’t tumor cells and tumor stem cells tend to escape the body’s immune surveillance? Then, special methods are used so that the immune system can find these mutated cells and allow lymphocytes (T cells or NK cells) to directly address them in situ, which is immunotherapy.
In immunotherapy for hematopoietic malignancies, nothing is more inspiring than CAR-T. T cells are the fiercest “hunters” in the immune system. They use their receptors to sense cells with specific proteins on their surface, and in this way target abnormal cells and remove them.
The human battle against tumors continues.