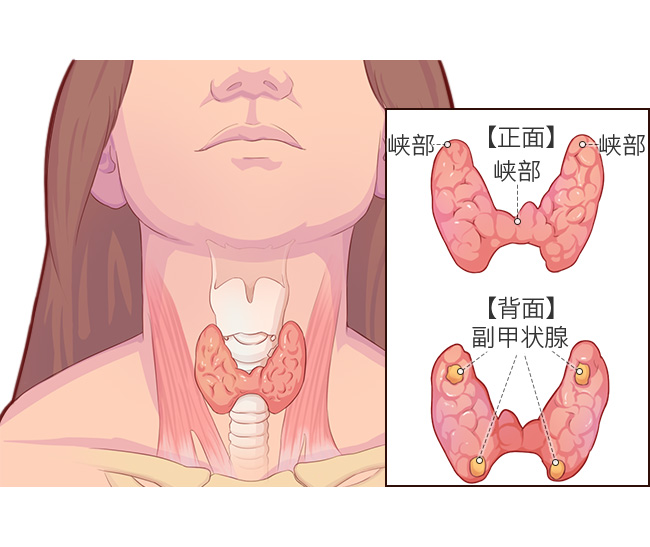
The thyroid is a butterfly-shaped gland located at the front of our neck. Thyroid cancer, a malignant tumor that develops from the cells of the thyroid gland.
What types of thyroid cancer are classified
The World Health Organization (WHO) classifies thyroid cancer into four categories:
- Papillary carcinoma
- Papillary thyroid carcinoma (PTC)
- Papillary thyroid carcinoma (PTC)
- follicular thyroid carcinoma (FTC)
- Medullary thyroid cancer (MTC)
- anaplastic thyroid cancer (ATC)
These four categories cover more than 95% of all thyroid cancers. Of these, papillary and follicular carcinomas are together called differentiated thyroid cancer.
Related reading:
Different types of thyroid cancer have different characteristics, as detailed in the table below
|
Table 1. Characteristics of the four major types of thyroid cancer |
||||
| Type | Percentage | Population with good prevalence | Clinical features | Outcome |
| Papillary carcinoma | About 80% | 20 to 40 years old, more common in women | There are usually no obvious symptoms in the early stages, but hoarseness and dyspnea may occur in the later stages | Lower malignancy, 10-year survival rate of 90%, easy recurrence |
| Follicular carcinoma | 10% to 15% | around age 50 | Usually asymptomatic nodules, which can present later with symptoms such as hoarseness and dyspnea | Moderately malignant, the prognosis is not as good as for papillary carcinoma, with 10-year survival rates of 98%, 88%, and 56% for patients in the low-, intermediate-, and high-risk groups, respectively. |
| Medullary carcinoma of the thyroid | 5% | Any age, common between 50 and 60 years, similar proportion of men and women | Neck lumps, facial flushing, palpitations, diarrhea, and wasting | Moderate malignancy, with 10-year survival rates averaging 50% to 90%. |
| Undifferentiated carcinoma of the thyroid | 5 % or so | around 70 years old | presenting with a rapidly growing mass in the neck with local compression symptoms such as dyspnea, dysphagia, hoarseness | Highly malignant, with a one-year survival rate of 5% to 15%. |
Recognizing rare thyroid cancers
In addition to the four common types mentioned above, thyroid cancer includes many rare types, and their characteristics are summarized in the table below.
|
Table 2. Characteristics of rare types of thyroid cancer |
|||
| type | Population | Clinical features | Outcome |
| Hürthle cell carcinoma | Female and over 50 years | More aggressive and more likely to metastasize distantly | Poorer |
| Primary squamous cell carcinoma of the thyroid |
Elderly, more commonly in women |
Tumor is rapidly enlarging, with significant signs of compression, and lymph node metastases may occur | Highly malignant, aggressive, poor outcome, 5-year survival rate less than 50% |
| Mixed medullary-filtrating carcinoma of the thyroid |
Similar to medullary carcinoma, occurring at any age and in similar proportions in men and women |
Lymph node and distant metastases, along with elevated blood calcitonin levels | Moderate malignancy with 10-year survival rates averaging over 50% to 90% |
| Primary mucinous epidermoid carcinoma of the thyroid | Female | Early presentation is mostly asymptomatic thyroid nodules, with corresponding presentation in later stages due to external invasion and compression. | Low malignancy, with a 5-year survival rate of nearly 90% |
| Intra-thyroidal thymic carcinoma | Middle-aged and elderly | Longer, slower progressive disease, often presenting as a painless nodule followed by symptoms such as tracheal compression or hoarseness | Better outcome |
| Sclerosing mucinous epidermoid carcinoma with eosinophilia | Adults, more common in women | Progressively enlarging neck mass with a tendency to extrathyroidal invasion | About half of patients have a disease-free survival of 3 months to 9 years, and half have local recurrence or distant metastases |
| Primary mucinous thyroid cancer | Unclear | High incidence of lymph node metastasis, susceptible to distant metastases, and rapid progression | Poor outcome |
|
Note: Calcitonin (CT) is a common blood marker used to detect and follow up medullary carcinoma. |
|||
Co-written by Dr. Tingting Zhang, Cancer Hospital of Fudan University