Acute myeloblastic leukemia (AML), also known as acute myeloid leukemia, is a hematologic neoplasm that usually begins in bone marrow cells that have not yet differentiated into leukocytes. However, in some cases AML may also originate from other types of hematopoietic cells.
While no cure has been achieved, the use of different treatment regimens will make a very large difference in clinical outcomes.
Pathogenesis
Acute myeloid leukemia arises from the bone marrow tissue, which is the soft tissue inside the bone.
In patients with acute leukemia, bone marrow cells become diseased and do not differentiate cells according to the normal pathway. These undifferentiated cells, often referred to as mother cells, accumulate in the bone marrow tissue.
Acute myeloid leukemia is sometimes referred to as:
- Acute granulocytic leukemia
- Acute non-lymphoblastic leukemia
If left untreated, acute myeloid leukemia can quickly become life-threatening. Because this is an “acute leukemia,” it can spread rapidly to the blood and other parts of the body, such as:
- Lymph nodes;
- liver;
- Spleen;
- brain and spinal cord;
- Testes.
Every patient is different, and the course of AML depends on certain specific factors, including response to therapy. The outcome of treatment may be relatively positive if the patient is accompanied by:
- Age less than 60 years;
- Relatively low white blood cell count levels when the patient is diagnosed;
- No previous history of blood disorders or cancer;
- No specific genetic mutations or chromosomal abnormalities associated with the disease.
Cause of pathogenesis
The specific etiology of patients with acute myeloid leukemia is not known. However, certain conditions are known to be “risk factors” for the development of the disease. Patients are more likely to develop the disease when they have the following conditions:
- Smoking;
- Exposure to certain chemicals, such as benzene (a solvent used in oil refineries and other industrial processes and also found in cigarette smoke), certain cleaning products, detergents, and paint strippers;
- The use of certain chemotherapy drugs used to treat other cancers, such as nitrogen mustard, methylbenzylhydrazine, and nitrogen mustard phenylbutyrate, especially when combined with radiation therapy, carries a higher risk;
- Exposure to high doses of radiation;
- Concomitant with certain blood disorders such as myeloproliferative disorders (e.g., chronic granulocytic leukemia);
- with certain congenital defects and disorders, such as Down syndrome;
- Male.
Symptoms
Acute myeloid leukemia begins in the bone marrow – the spongy soft tissue within the bone where blood production occurs. The disease will inhibit undifferentiated bone marrow cells from continuing to form healthy blood cells.
The body has three main types of blood cells:
- White blood cells fight infection;
- Red blood cells carry oxygen throughout the body;
- platelets help blood to clot in case of injury.
Early symptoms
In the early stages of acute myeloid leukemia, patients may feel as if they have the flu or other illnesses because their bodies produce fewer healthy blood cells.
Related symptoms may include:
- Lethargy;
- fever;
- loss of appetite;
- weight loss;
- Extensive sweating at night.
There are many other causes of these symptoms, so patients need to work with their doctors to find the exact cause.
Symptoms of different disease types
There are several clinical types of acute myeloid leukemia, each originating from a different blood cell. Therefore, the patient’s symptoms depend on the specific type of cells that initiated the lesion.
If a patient has a lower than normal number of healthy red blood cells, the following symptoms may occur:
- Lethargy;
- weakness;
- pale complexion;
- Irregular heart rhythm;
- Dizziness;
- Cold hands and feet;
- Shortness of breath;
- Headache;
- Weight loss;
- Loss of appetite.
If a patient’s white blood cell count is below normal, the risk of infection is significantly higher. Also, it takes a long time for the infection to get better after it occurs. Infections may cause the following symptoms:
- fever;
- Weakness;
- muscle pain;
- Fatigue;
- Diarrhea.
If a patient’s platelet count is below normal, then it is difficult for the blood to clot when an injury occurs. The following symptoms may occur:
- Frequent bruising;
- Bleeding profusely;
- bleeding gums;
- Red spots under the skin from bleeding;
- Nose bleeding;
- Skin ulcers that do not heal.
Symptoms of cancer after it has spread
Leukemia cells can spread to other parts of the body and cause the following symptoms:
- Difficulty maintaining body balance;
- Blurred vision;
- Bone and joint pain;
- Numbness of the face;
- Twitching throughout the body;
- A rash;
- Swelling in the abdomen;
- Swollen and bleeding gums;
- swelling of lymph nodes in the neck, groin, axilla, or above the collarbone.
If a patient has any of these symptoms, he or she should go to the hospital. Although it may be caused by an illness like the flu, it is best to get a thorough checkup just in case. The doctor will ask the patient exactly what symptoms are present and how long they have lasted, and may need to perform blood tests and other types of clinical tests to confirm the final diagnosis of AML.
Complications
Because acute myeloid leukemia severely affects the healthy blood cells in the patient’s body, it may lead to the following complications:
Anemia
Patients lack sufficient red blood cells, whose important role is to transport oxygen to organs and tissues throughout the body. When a patient becomes anemic, they do not get enough oxygen to all parts of the body. Subsequently, the patient feels tired, weak, and has difficulty breathing.
Bleeding
If a patient’s platelet levels are reduced, the blood has difficulty clotting when they are injured. The risk of daily bruising or bleeding is also increased, and bleeding can be difficult to control when the skin is injured by a sharp object or when the nose bleeds. Patients may also experience internal bleeding, which can be a very serious condition.
Low immune system function
White cells in the immune system normally recognize and attack invading pathogens. When acute myeloid leukemia occurs, the patient will lack enough healthy white blood cells to fight an exogenous infection.
If the patient’s immune system is low, the risk of infection rises significantly. Patients will also have a prolonged recovery time after an infection occurs.
To avoid infections, doctors ask patients to stay away from anyone with an infectious disease and to take regular prophylactic antibiotics. Timely vaccination can also help protect against common pathogens, but patients may not be candidates for “live attenuated” vaccines, such as the shingles vaccine. The doctor will talk to the patient in detail and recommend the latest type of vaccine that is appropriate for the patient.
Diagnosis
Diagnosis
If a patient develops fever, shortness of breath, unusual bruising or bleeding, it may be a sign of AML and should be seen at the earliest possible time.
Patients need to be seen in an oncology or hematology specialty for leukemia-related care. The doctor will first perform clinical testing to determine if the patient has acute myeloid leukemia and its specific type. The better the doctor understands the patient’s condition, the better the chance of successful treatment.
Physical examination
At the time of the patient’s visit, the doctor will ask about general health. During the exam, the doctor will look for signs of leukemia, such as sternal pressure and bruising or bleeding spots under the skin.
Acute myeloid leukemia testing
Patients with acute myeloid leukemia are due to a lesion in the stem cells. Stem cells are located in the bone marrow, the spongy soft tissue inside the bone, and can differentiate to produce white blood cells, red blood cells, and platelets. When a patient develops the disease, the stem cells are unable to produce healthy blood cells due to genetic mutations.
The following tests can be used to identify the presence of undifferentiated abnormal blood cells in the blood and bone marrow:
- Blood sample testing;
- Bone marrow examination;
- Lumbar puncture;
- Imaging;
- Cytogenetic and molecular biology genetic testing.
Blood testing
For blood testing, the nurse first draws a blood sample from a vein in the patient’s arm using a needle. Subsequently, different types of tests are used to inform the diagnosis of acute myeloid leukemia:
- Complete blood count (CBC): Assesses the level of white blood cells, red blood cells, and platelets in the patient’s blood. If the patient has acute myeloid leukemia, the patient’s white blood cell level will rise and the levels of blood cells and platelets will fall.
- Peripheral blood smear: The doctor looks at the patient’s blood sample through a microscope to assess the number, shape, and size of the white blood cells and to look for the presence of undifferentiated mother cells in it.
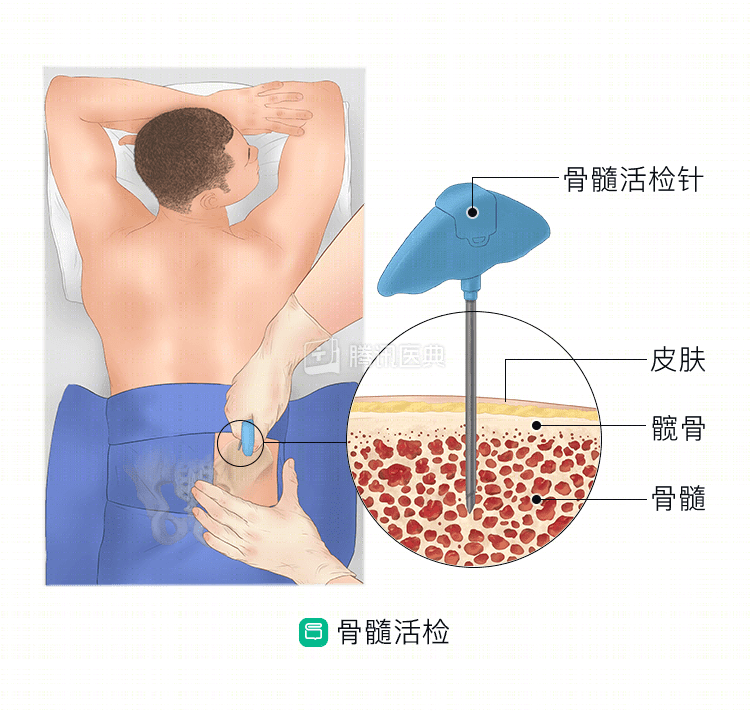
Bone marrow examination
To reach a definitive diagnosis, the patient also undergoes a bone marrow test. The doctor will use a puncture needle to extract a small amount of bone marrow or a small piece of bone marrow tissue from the patient’s iliac bone.
The bone marrow sample is then sent to the laboratory for testing, where the pathologist looks at the patient’s blood cells through a microscope. If the patient’s bone marrow sample has more than 20% undifferentiated mother cells, the diagnosis of acute myeloid leukemia can be made.
Lumbar puncture (spinal tap)
In this test, the doctor uses a puncture needle to draw a small sample of cerebrospinal fluid (CSF) from the patient. The doctor examines the CSF sample under a microscope for the presence of leukemia cells.
Imaging
Imaging is the use of radiation, sound waves, and magnetic fields to image organs in the patient’s body. Acute myeloid leukemia does not show formed tumor tissue on imaging scans, but clinicians can use such tests to see if a patient has an infection or other complications due to the leukemia.
The following imaging tests help physicians diagnose and evaluate acute myeloid leukemia:
- CT scan: A CT scan uses X-rays to image the patient’s body in high definition. CT scans can show if AML has caused the patient’s spleen or lymph nodes to swell. Before the test is performed, the patient may need to be given a special contrast agent by mouth or intravenously. This developer helps the doctor see the condition of the organs in the body more clearly during the scan.
- Ultrasound: Sound waves are used to look at the patient’s lymph nodes, liver, spleen, and kidneys to see if they are enlarged.
- X-rays: Use low-dose radiation to image organ tissue in the patient’s body. Your doctor may order an x-ray chest x-ray to look for lung infections.
Cytogenetic and genetic testing
Acute myeloid leukemia includes several types. Clinicians can identify the specific type of lesion in a patient by identifying cytogenetic and genetic variants in cells from blood or bone marrow samples. This will help the clinic develop the most effective treatment plan.
Genetic testing includes:
- Cytogenetic analysis looks for chromosomal changes in the patient’s leukemia cells. Chromosomes are made up of DNA, and in some patients with acute myeloid leukemia, an exchange of DNA fragments between two chromosomes occurs, known as chromosomal translocation.
- Immunophenotypic testing looks for surface markers of leukemic cells. Different types of leukemia cells have their own unique markers.
- Fluorescence in situ hybridization (FISH) uses special dyes to label specific sites of chromosomes to look for abnormal chromosomes in a cell sample.
- Polymerase chain reaction (PCR) uses a chemical reaction to detect the presence of genetic mutations in a cell sample.
Treatment
Acute myeloid leukemia drives the bone marrow to produce large numbers of abnormal blood cells. These diseased cells crowd out healthy red blood cells, white blood cells, and platelets. The treatment plan for acute myeloid leukemia is to remove the diseased cells from the bone marrow and blood. The goal is to put the patient into remission and for the symptoms associated with leukemia to disappear completely.
There are several different therapies that can be used to treat acute myeloid leukemia:
- chemotherapy;
- stem cell transplantation;
- radiotherapy;
- Targeted therapy.
Patients are treated in 2 phases:
Phase 1: Induction of remission therapy.
Patients begin high-dose chemotherapy to kill as many leukemia cells as possible. Hospitalization may be required for 4 to 6 weeks so that the physician can closely monitor the patient and promptly manage the various side effects of the chemotherapy drugs. Targeted therapy drugs may also be given in combination.
At the end of treatment, the patient’s bone marrow begins to produce healthy blood cells. The doctor will take a sample of the patient’s bone marrow to see if there are still leukemia cells left in the blood system. If no leukemia cells are detected, the doctor will call the patient “in remission. After that, the patient needs intensive post-remission treatment to ensure that the disease remains in remission for a long time.
Phase 2: Post-remission treatment.
Post-remission therapy will use a more intense regimen to destroy any remaining tumor cells. There are 3 main options:
- Chemotherapy: Medium- to high-dose chemotherapy is given once a month for 6 to 8 doses.
- Allogeneic stem cell transplantation: transplantation of stem cells from volunteer donors.
- Autologous stem cell transplantation: Stem cell transplantation from the patient’s own stem cells.
Chemotherapy
The use of potent chemotherapy drugs to kill tumor cells throughout the body. Patients can be given the drug orally, intravenously, or subcutaneously.
If the tumor spreads, patients also need to have chemotherapy drugs injected into the fluid around the brain and spinal cord, which is clinically known as intrathecal chemotherapy.
Chemotherapy kills rapidly dividing cells in the patient’s body, such as tumor cells, but it also affects other rapidly dividing cells in the body – such as those in the immune system, mouth, intestinal wall, and hair follicles.
When chemotherapy drugs damage such healthy cells, the following side effects can occur:
- nausea and vomiting;
- Hair loss;
- Mouth ulcers;
- Fatigue;
- Loss of appetite;
- Diarrhea, constipation;
- easy bruising or bleeding;
- Rising risk of infection.
The vast majority of these side effects go away on their own once the patient has finished treatment. During treatment, doctors may also give patients medications or take other steps to help control the side effects of chemotherapy.
Stem cell transplantation
The higher the dose of chemotherapy a patient receives, the more tumor cells are killed. However, high-dose chemotherapy can also damage the bone marrow, causing blood cell levels to drop to dangerous levels.
Doctors can perform a stem cell transplant at the end of a patient’s high-dose chemotherapy, replacing the bone marrow cells that were severely damaged during treatment with the patient’s own stem cells or those donated by a donor. Such transplanted stem cells will gradually differentiate and form new healthy blood cells.
There are 2 types of stem cell transplantation methods available:
- Allogeneic stem cell transplantation: Using donor-donated stem cells, this is the most common type of stem cell transplant. Close relatives such as parents, brothers or sisters, for example, are the best stem cell donors. The main risk of allogeneic transplantation is graft-versus-host disease, in which the cells provided by the donor recognize the patient’s body as exogenous and therefore attack organs and tissues everywhere. Symptoms include rash, itching, nausea, diarrhea, mouth ulcers, and jaundice (yellowing of the eyes and skin).
- Autologous stem cell transplantation: Stem cells are collected from the patient’s bone marrow or blood and frozen for preservation before the patient undergoes chemotherapy. Subsequently, after the patient has completed high-dose intensive therapy, they are then transfused back into the patient’s body. Because these stem cells come from the patient themselves, no rejection occurs. The disadvantage is that it is difficult to completely separate the leukemia cells from the healthy stem cells, and it is likely that some leukemia cells will be mixed in during the stem cell transplant and eventually be infused back into the patient at the same time.
.
After completing the stem cell transplant, the patient must be hospitalized for a period of time for observation and timely management of associated treatment side effects. Because this regimen involves very high doses of chemotherapy, more serious complications can arise, such as:
- Very low normal blood cell counts, causing patients to have a significantly higher risk of infection and bleeding;
- damage to the lungs, bones, and thyroid;
- Cataracts;
- Loss of fertility;
- The development of another type of cancer several years later.
Treatment of acute promyelocytic leukemia
Acute promyelocytic leukemia (APL) is a subtype of acute myeloid leukemia, but the clinical treatment varies. This is because these leukemia cells contain specific proteins that affect the way blood clots. When chemotherapy drugs kill leukemic cells, such proteins are released and can form dangerous blood clots or severe bleeding can occur in the body.
For patients with acute promyelocytic leukemia, drugs are needed to differentiate the leukemia cells into mature, healthy blood cells so they do not rupture and release proteins that interfere with clotting.
Two drugs that are commonly used to treat acute promyelocytic leukemia are:
- All-trans-retinoic acid (ATRA): Patients may need continuous treatment with this drug for 1 to 2 years. Major side effects include headache, fever, rash, mouth or throat ulcers, pruritus, and elevated cholesterol.
- Arsenic trioxide: Side effects include fatigue, nausea, vomiting, diarrhea, abdominal pain, cardiac arrhythmia, and nerve damage.
Patients may also be given the drug in combination with chemotherapy.
Radiotherapy
Radiotherapy uses high-energy radiation to kill tumor cells. Patients need radiation therapy to treat acute myeloid leukemia that has spread to the brain and spinal cord or spread to the bones. High-dose radiation therapy is also sometimes used before a stem cell transplant is performed. Usually adults are treated with external radiation, which is an instrument that emits radiation from outside the patient’s body.
Side effects from radiation therapy may include:
- Sunburn, redness and swelling of the skin;
- Mouth ulcers – radiotherapy to the patient’s head and neck;
- nausea, vomiting or diarrhea – radiotherapy to the patient’s abdomen;
- Fatigue;
- bleeding or bruising;
- Rising risk of infection.
Clinical trials
If none of the existing AML treatment options work, or if relapse occurs after treatment ends, another option for patients is to participate in a clinical trial of a new therapy.
In a clinical trial, patients have the opportunity to try treatment with a new drug that is not yet on the market. The physician will recommend the most appropriate clinical trial based on the patient’s specific condition and will provide detailed information about the details of the enrolled trial.