1. What is leukemia?
.
Leukemia is a malignancy in which blood cells are formed. The current incidence is essentially similar to that of the 1950s, although with the introduction of new treatment options, patients have longer survival periods than before and in some cases can even be cured.
Although it is the most common malignancy in children, there are actually more adult patients than pediatric patients. Leukemia includes several types, most of which originate from white blood cells. As for the progression of their disease, and the treatment options that patients need to receive vary widely.
2. Who is at risk for leukemia?
.
The exact cause of leukemia is not known, and chemicals present in cigarettes or used in industrial production, such as benzene, may increase the risk of developing it. Some chemotherapy drugs or radiation therapy used to treat cancer can also increase the risk of the disease.
In addition, other clinical risk factors include the presence of certain genetic disorders, such as Down syndrome and Fanconi anemia, or the presence of other family members, such as a parent, brother, sister, or child with leukemia.
3.
3. How are blood cells produced?
.
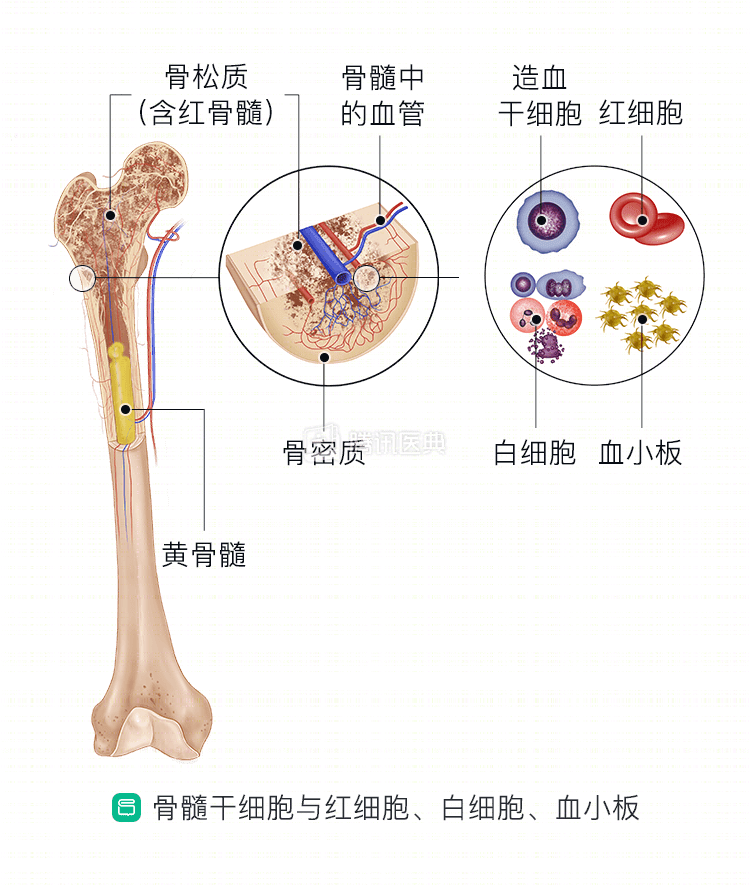
There are 3 main types of blood cells in the body: white blood cells that fight disease, red blood cells that deliver oxygen, and platelets that start the clotting process when the body is traumatized. They all originate in the body’s bone marrow stem cells, the spongy soft tissue located inside the bone that produces and releases large numbers of blood cells every day. Under normal circumstances, the blood system functions in an orderly manner. However, if leukemia occurs, the whole process becomes chaotic and disorganized.
4. How does leukemia occur?
It only takes a mutation in the DNA of a single blood stem cell to cause leukemia. DNA is fundamental to the proper functioning of the body, and even a small mutation can have a huge impact.
As the cells divide, the number of mutated cells increases exponentially, there are more and more cells with DNA mutations, and soon the patient will have a large number of abnormal blood cells.
They are unable to function properly, but occupy the bone marrow cavity, leaving healthy cells with no room to live. This is the main cause of clinical symptoms.
5. What are the signs of leukemia?
.
Leukemia has no signs of onset and the clinical presentation is often not obvious, and the initial symptoms may be similar to the flu.
- Red blood cell reduction causes anemia, and patients are pale, tired, and have difficulty breathing.
- With reduced levels of healthy white blood cells, they are unable to fight infections and will get sick more often and for longer periods of time.
- Lowered platelets, on the other hand, can make patients more prone to bruising and bleeding.
6. What are the symptoms of leukemia?
Patients may feel ill and weak, with chills, fever, and night sweats; they may also have nosebleeds, red spots on the skin, and swollen or bleeding gums. In addition, weight loss may be unexplained, and joints and bones may be damaged.
Leukemia cells may accumulate and cause swelling of the lymph nodes, spleen, and liver. If they accumulate in the patient’s brain, they can cause headaches, confusion, and generalized seizures.
7. How are leukemias classified?
.
Although leukemia can cause systemic abnormalities of the hematopoietic system, though it is named based on its leukocyte origin (myeloid or gonadal), and the rate of progression (acute or chronic).
Acute leukemia may develop within a few weeks when there are large numbers of abnormal mother cells in the bone marrow. Doctors usually test for acute leukemia when a patient develops an infection that is delayed in recovery. Chronic leukemia, on the other hand, progresses very slowly, and abnormalities are usually found incidentally during routine blood tests.
8. What are the common types of leukemia?
.
- Acute myeloblastic leukemia (AML) is the most common type of acute leukemia in adults.
- Acute lymphoblastic leukemia (ALL) is the most common type of acute leukemia in children.
- Chronic myelogenous leukemia (CML) is a hematologic neoplasm that is directly related to the development of DNA defects in the patient’s cells.
- Chronic lymphocytic leukemia (CLL) causes white blood cells to fail to enter the death process normally.
9. How is leukemia staged or graded?
.
Unlike other cancers, the grading of leukemia does not describe how far the tumor has spread; high-grade leukemia means that more aggressive treatment options are needed or that treatment is more difficult.
Chronic lymphocytic leukemia may be graded as low-risk, intermediate-risk (or standard), or high-risk; chronic myeloid leukemia has the lowest number of metaplastic cells in the chronic phase, an increased number of metaplastic cells in the accelerated phase, and more so in the acute phase; acute leukemia is difficult to stage because it progresses too rapidly.
10. How is leukemia diagnosed?
.
The first test is a complete blood count (CBC), which shows the number of different blood cells in the patient’s body. Often, the results of this test are almost clear enough to determine whether leukemia is present.
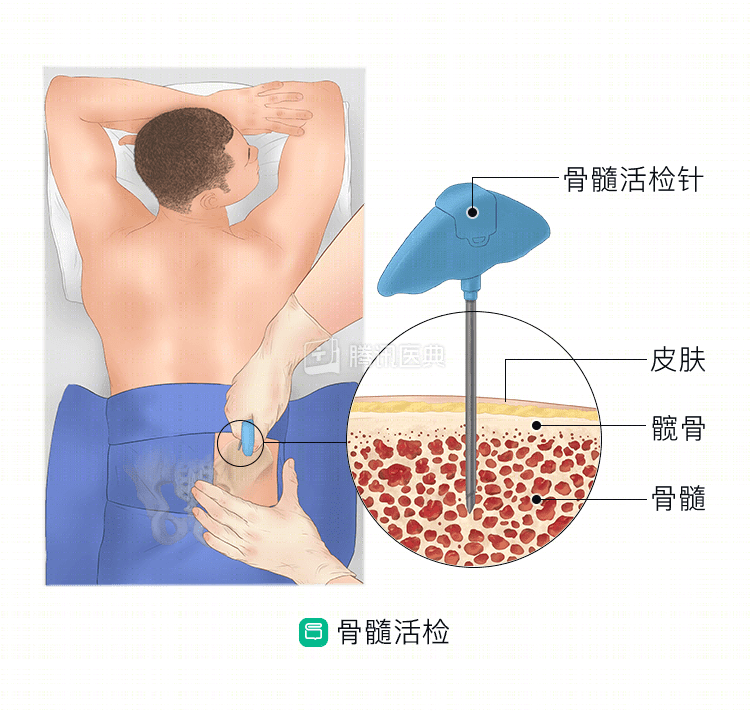
For further confirmation and more detailed information about the disease, a bone marrow biopsy is needed. Clinicians typically use a needle to collect a bone marrow sample from the patient’s iliac bone for pathologic testing.
Both of these tests can also be used to assess a patient’s response during treatment.
11. What tests are available for leukemia?
.
In order to develop an optimal treatment plan, the physician needs to have an in-depth understanding of the patient’s specific condition.
- A blood smear test can show the number of mother cells in the patient’s body, and their morphological characteristics.
- Molecular biology testing can provide insight into the DNA variation of leukemia cells.
- Imaging tests, such as CT, MRI, and ultrasound scans, can be performed to look for signs of cancer in the lymph nodes and organs of the patient’s body.
- A lumbar puncture allows assessment of whether leukemia cells have spread to the patient’s brain and spinal cord.
12. Can chemotherapy treat leukemia?
.
Chemotherapy is the standard treatment option for acute leukemia. Chemotherapy regimens attack leukemia cells throughout the body with drugs, and the effects of the first cycle of chemotherapy can last for several weeks. Once the leukemia goes into remission, patients usually undergo subsequent cycles of chemotherapy for the next 4 to 8 months. For some types of leukemia, patients will need subsequent cycles of chemotherapy over the next 2 to 3 years.
During treatment, antiemetics are prescribed to help with the side effects of chemotherapy drugs.
13. What is a stem cell transplant?
.
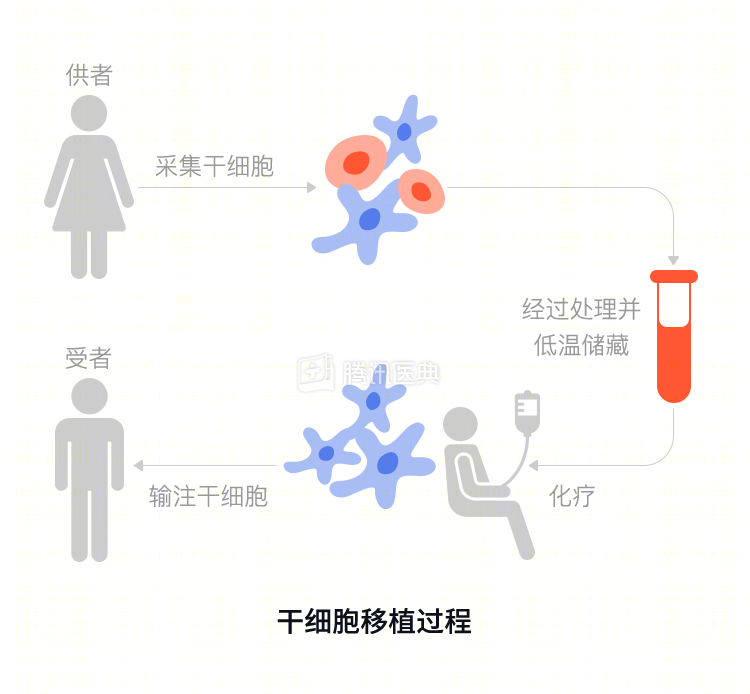
The higher the dose of chemotherapy drugs, the more leukemia cells are killed, but also the healthy normal cells are killed. At this point, the leukemia patient needs a stem cell transplant from a volunteer donor to restore blood production in the body.
However, there are some risks associated with this therapy because the immune system in the patient’s body may reject the transplanted stem cells. Therefore, this option is mainly used when other treatments have failed. Although, stem cell transplants can sometimes cure leukemia, they can also be fatal to the patient’s immune system.
14. What is targeted therapy?
.
These drugs are usually used to treat chronic leukemia. Because there are significant differences between leukemic and normal cells, targeted drugs will only recognize and attack leukemic cells and will not affect healthy cells. Tyrosine kinase inhibitors (TKIs) can essentially achieve a cure for chronic myeloid leukemia, but patients may need to take the drugs for life.
For chronic lymphocytic leukemia, monoclonal antibody drugs can be used to target the leukemia cells directly so that the body’s immune system can kill them. Kinase inhibitors, on the other hand, are effective in stopping the diseased cells of chronic lymphocytic leukemia from continuing to grow and divide.
15. What is gene therapy?
.
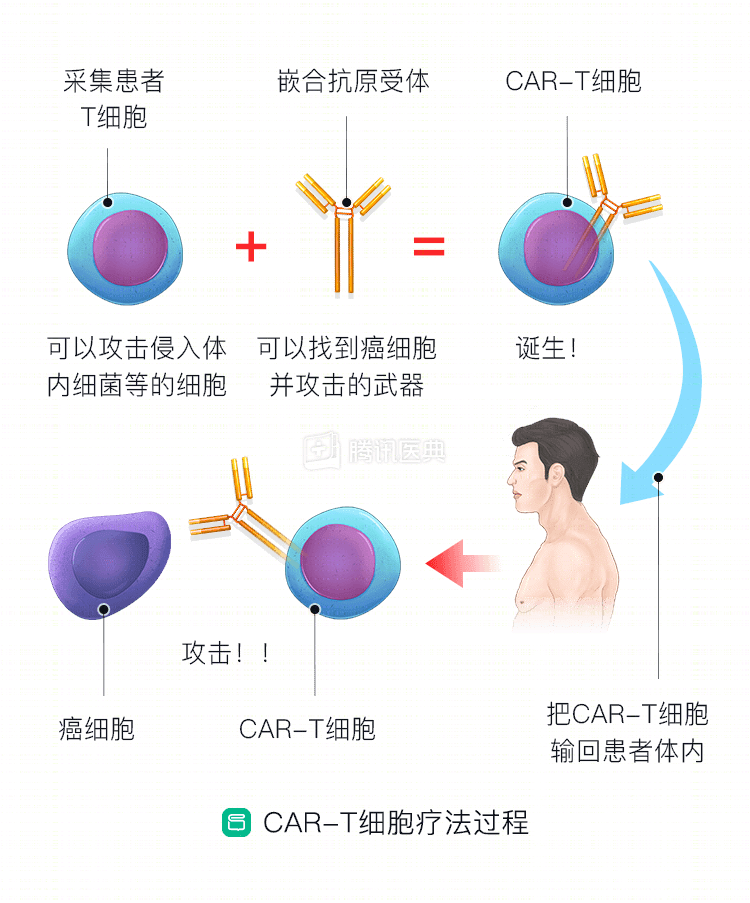
CAR T is a new type of individualized immunotherapy. During the treatment process, the patient’s T cells are first collected and sent to a laboratory to add new genes to the T cells so that they can target and kill specific leukemia cells once they enter the patient’s body. These modified T cells are then infused back into the patient.
However, this treatment is currently only available for younger and pediatric patients with B-cell acute lymphoblastic leukemia that has failed to respond to treatment or has relapsed.
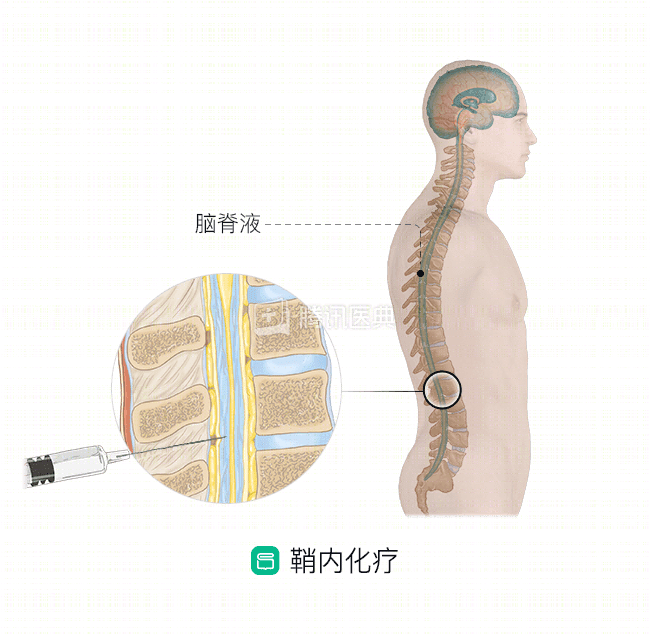
16. How do you protect the patient’s brain and spinal cord?
.
This is a clinical issue of concern to both doctors and patients. Although leukemia does not originate in the central nervous system, it will eventually spread there in at least half of patients. To prevent this, physicians inject chemotherapy drugs directly into the patient’s myelin sheath and may need to administer the drugs multiple times.
17. What is watchful waiting?
.
For many types of leukemia, patients must start treatment right away. But for chronic lymphocytic leukemia, medication is usually not needed until symptoms appear. Patients just need regular follow-ups and routine checkups to closely monitor their progress. Some patients may not even experience any symptoms for the rest of their lives, maintaining a normal life.
Treatment needs to be started if a patient’s white blood cell levels begin to rise substantially, platelet levels fall substantially, or symptoms such as enlarged lymph nodes develop.
18. What do I need to be aware of during treatment?
.
Both leukemia and its treatment can cause a decrease in the number of healthy blood cells. To help patients complete treatment successfully, blood transfusions may be given during this time to improve anemia, antibiotics to control infections, and platelet transfusions to treat clotting disorders. In addition, because patients are at high risk for infection, both patients and close contacts need to wash their hands frequently.
19. How long can I live if I have leukemia?
.
There are many factors that affect survival, including the type of leukemia, how far the disease has progressed, and the patient’s overall health status. And the clinical statistic of survival is an overall average; it does not determine the survival of a particular patient.
The 5-year relative survival rate for leukemia is about 60%. This means that for every 10 people with leukemia compared to 10 people without leukemia, an average of 6 people with leukemia are still alive after 5 years.
20. What are the characteristics of childhood leukemia?
.
About 3/4 of all pediatric leukemia patients have acute lymphoblastic leukemia, with the remainder having mostly acute myeloid leukemia. Chronic leukemia is very rare in pediatric patients.
Acute lymphoblastic leukemia is usually successfully cured, in part because the child responds well to treatment. The entire course of treatment may take 2 to 3 years, but eventually almost all children – about 9/10 – are completely cured. Pediatric patients with acute myeloid leukemia also have a higher success rate than adult patients.
21. How are patients with leukemia followed up?
.
Whether a patient is in remission, on watchful waiting, or on ongoing treatment, it is important to remember to follow up regularly and monitor closely. It is necessary for patients to communicate and interact fully with their physicians, not only about changes in their condition or symptoms, but also about changes in mood during treatment and daily distress. Patients can also consult with their physicians about how they can participate in a long-term care plan that will both meet their follow-up medical needs and effectively improve their quality of life.
22. Can leukemia be prevented?
.
There is a lack of effective means to prevent leukemia, and no effective screening for the disease has been identified.
Staying away from tobacco, benzene, and high doses of radiation may help reduce the risk of developing the disease. Otherwise, the best thing to do is to get an annual checkup, where your overall health can be examined in detail, including routine hematology tests that can detect abnormalities early.