Leukemia is a hematopoietic malignancy with a very high mortality rate, and the vast majority of subtypes remain incurable. The current primary treatment is cytotoxic drug chemotherapy combined with hematopoietic stem cell transplantation, which has improved survival in some patients.
However, most patients remain at risk of relapse and refractory to treatment due to the small variety of chemotherapeutic agents and lack of targeting, which can easily lead to drug resistance and patient intolerance.
What is relapse?
A relapse is when leukemia cells are detected again in the bone marrow, or when leukemia cells invade other parts of the body and develop a mass. After complete clinical and hematologic remission with chemotherapy, 10 to 10 residual leukemia cells remain in the body, which are called minimal residual disease (MRD).
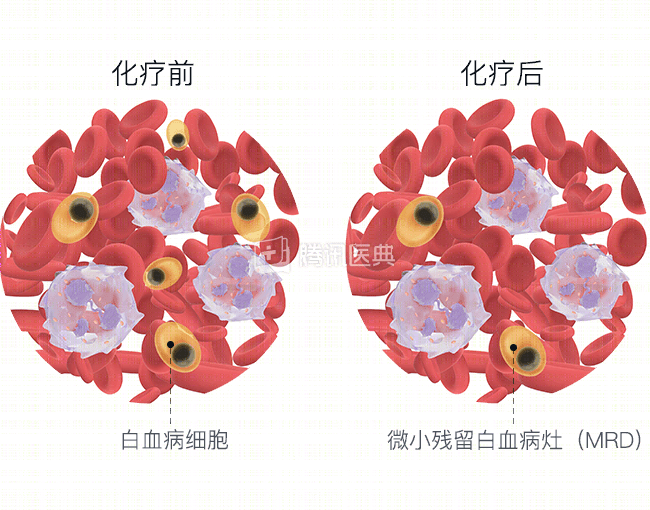
Because the current means of detecting MRD is limited, even if no leukemia cells are detected as remaining, it does not mean that there are no leukemia cells in the body. MRD is a major cause of leukemia recurrence.
What happens after a relapse?
For patients with relapsed leukemia, there is a distinction between recent relapse, which is less than 6 months, and distant relapse, which is greater than 6 months. Once relapsed, molecular and cytogenetic risk stratification needs to be performed again, with recent relapses requiring combination therapy with unused agents and distant relapses allowing for re-induction by evaluating previously sensitive agents.
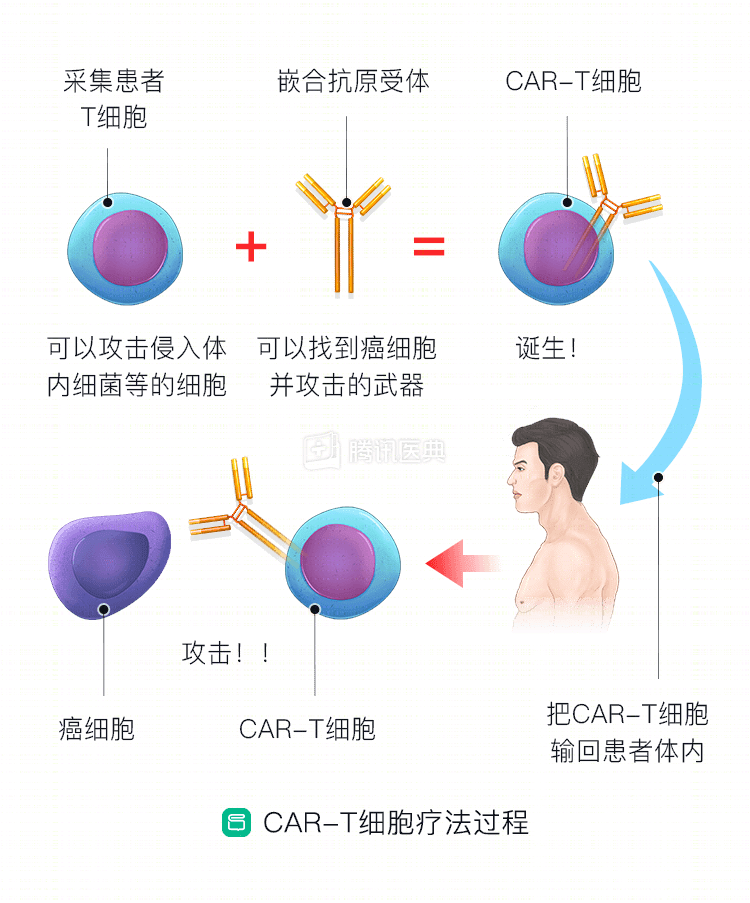
Once there is a first relapse, many patients will have recurrent relapses with increasingly shorter intervals, so try to choose the right time for intensive therapy such as transplantation or CAR-T, if available.
At relapse of acute promyelocytic leukemia (APL), which is currently very well treated, and at progression of chronic granulocytic leukemia, very highly targeted arsenite/ATRA, novel tyrosine kinase inhibitors for re-induction, and APL must be performed for meningeal leukemia prophylaxis. Only in cases of recurrent refractory relapses or clinical drug intolerance should we consider adding clinical studies or allogeneic hematopoietic stem cell transplantation.
Patients with acute myeloid leukemia, lacking targeted therapeutic agents, should be considered for chemotherapy regimen selection based on a combination of genetic factors, time to relapse, individual patient (e.g., age, physical status, comorbidities, early treatment options), and the patient’s willingness to be treated. Depending on the specific genetic and chromosomal alterations, treatment can be combined with appropriate epigenetic modulation (decitabine, azacitidine) or clinical trials of targeted agents (FLT3-ITD mutation inhibitors, CAR-T, etc.). In younger patients (<60 years of age), HSCT is feasible if conditions allow.
For acute lymphoblastic leukemia, the use of tyrosine kinase inhibitors can be adjusted if Philadelphia chromosome positive (Ph+). The choice of salvage chemotherapy regimens (Hyper-CVAD, etc.), enhanced chemotherapy in combination with drugs such as pemantel, and simultaneous aggressive preparation for allogeneic hematopoietic stem cell transplantation for transplantation as soon as possible after achieving complete remission. The use of CAR-T in B-cell leukemia has also yielded good results in recent years.