Surgery is still the primary treatment for thyroid cancer that has returned
Recurrence of thyroid cancer often occurs at the primary tumor, or in the lymph nodes of the neck, so the treatment of choice is surgery again.
Papillary and medullary carcinomas are prone to lymph node metastases, and when reoperation is performed, the surgeon will do a lymph node dissection of the affected side of the neck.
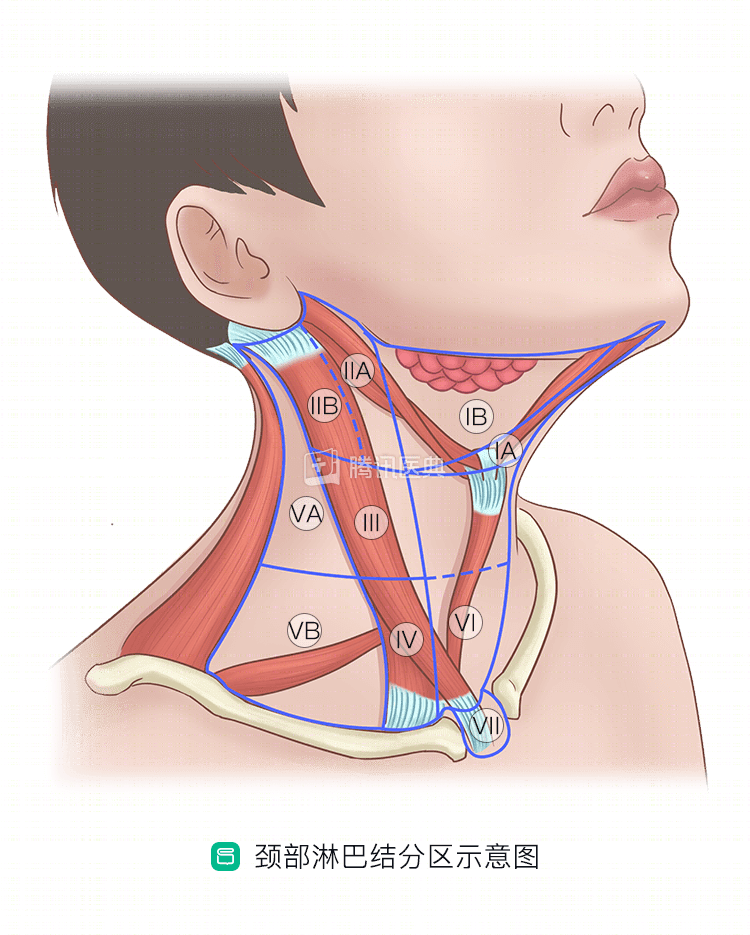
If there is no metastasis in the neck lymph nodes, do you need to do a lymph node dissection for reoperation? The medical community has not yet reached a consensus. The author’s hospital, Fudan University Cancer Hospital, would recommend lymph node dissection in region VI for these patients. The main considerations are:
- The high rate of lymph node metastasis is influenced by the anatomic site and not easily detected by routine examination;
- Area VI, if reoperated, can easily damage important structures such as the recurrent laryngeal nerve;
- Mapping the lymph nodes in area VI will help doctors consider further treatment options.
Some factors may “plant the seeds” for relapse, such as:
- Are already having cervical lymph node metastases, extra-thyroidal invasion, or distant metastases at the time of surgery
- A family history of thyroid cancer
- Surgery with residual cancer foci
Patients with these high-risk factors for recurrence and with an iodine uptake rate of more than 1% on a radioactive iodine scan have a better outcome with total thyroidectomy and postoperative radioactive iodine (RAI) therapy.
To summarize,in the case of recurrent highly differentiated carcinoma (papillary and follicular), doctors usually recommend total thyroidectomy followed by RAI therapy. However, undifferentiated and medullary carcinomas have very poor iodine uptake and are not candidates for RAI, and your doctor may recommend chemotherapy and/or radiation therapy.
When should I have surgery again?
If you are physically able, it is best to have surgery as soon as possible (within 1 week) after a recurrence is detected, or 3 months after the edema in the surgical area has resolved. In addition, the extent of resection in the first surgery has an impact on the timing of reoperation, and if the first surgery did not involve the recurrent laryngeal nerve and parathyroid area, reoperation can be advanced. If the first surgery damaged the recurrent laryngeal nerve, the surgeon will observe the recovery of the nerve and delay the reoperation as appropriate.
What are the risks of reoperation?
If only part of the thyroid was removed in the first surgery and the recurrence is followed by another surgery to remove the other side of the thyroid, the risk is lower because the target area is different between the two surgeries.
But if you operate again in the area of the previous surgery, the scarring and adhesions formed from the previous surgery alter the anatomy of the surgical area, making it difficult for the surgeon to find important structures such as the recurrent laryngeal nerve and parathyroid glands, increasing the risk of injury and the risk of intraoperative and postoperative complications.
Related reading:
Co-written by Dr. Shuwen Yang, Fudan University Cancer Hospital