What is lumpectomy thyroid surgery?
Lumpectomy, a procedure in which devices such as light sources, cameras, and surgical instruments are inserted through smaller surgical incisions, and the surgeon performs the procedure based on images transmitted to a monitor.
Endoscopic thyroid surgery (ETS) has been in development for more than 20 years and can perform thyroidectomy, central lymph node dissection, and other operations. There are two broad categories:
- Total lumpectomy without incision in the neck
- Lumpectomy-assisted thyroid surgery with small incisions in the neck (also called Miccoli surgery), which is assisted by lumpectomy techniques to shorten the incision of open surgery and reduce the surgical scar without compromising the outcome.

Lumpectomy for thyroid cancer, is it reliable?
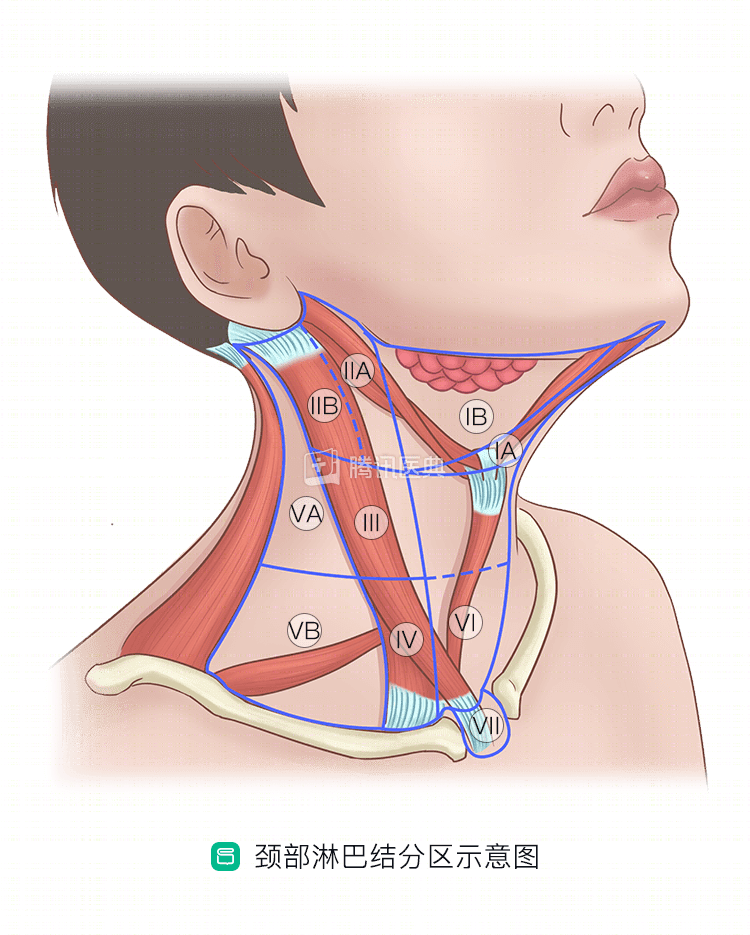
The biggest advantage of lumpectomy is that it is minimally invasive, reduces surgical scarring in the neck, and provides faster recovery after surgery. However, it has some limitations, as there are some “blind spots” in the lumpectomy, such as the lymph nodes in the VII region.
The ability of ETS to cure thyroid cancer is controversial and needs to be chosen carefully on a patient-by-patient basis. In addition, lumpectomy is more technically demanding for the surgeon and more expensive.
Which patients are candidates for lumpectomy? Which ones can’t?
Not all patients need or are able to undergo ETS, and according to the consensus of national and international experts, lumpectomy is recommended when the following 5 conditions are met.
- Age 15 to 45 years;
- Malignant tumor ≤ 2 cm in diameter without invasion of adjacent organs;
- No widespread lymph node metastasis and no fusion of metastatic lymph nodes;
- No superior mediastinum (the upper mediastinum).
- No lymph node metastasis in the upper mediastinum (region Ⅶ above);
- The patient had a strong desire for cosmesis.
Lumpectomy cannot be performed if the following conditions exist.
- Have severe coagulation disorders, cardiopulmonary dysfunction, and cannot tolerate general anesthesia and surgery;
- Has had surgery or radiotherapy to the neck;
- Second surgery for thyroid cancer.
How lumpectomy for thyroid cancer is done
ETS There are several modalities, the main ones include:
Transthoracic breast approach
This is by far the most common type of procedure, with the incision in the areola. It provides the surgeon with a surgical view similar to that of open surgery and is easy to perform.
It has the advantage of no neck scar, small incisional scar on the chest that is easily concealed, and the ability to perform bilateral glandular lobe surgery simultaneously. However, because of the occlusion of the sternum and bilateral clavicular head, there is a blind area for lymph node clearance in the VI region, which can easily result in residual lymph nodes in the VI region and increase the risk of recurrence. Therefore, if a patient has significant central zone lymph node metastases, the surgeon will choose this procedure with caution.
Transcatheter natural lumen
The most representative is the transoral approach, where the incision is located in the oral cavity.
It has the advantages of no scarring of the body surface, excellent healing of the oral mucosa, resulting in less injury, faster recovery, early postoperative showering of the entire body, and fuller exposure of the lymph nodes and the laryngeal retrolaryngic nerve in the central region.
But because the incision is in the oral cavity, there may be an increased chance of infection. In addition, the narrow operating space for the surgeon makes the procedure more difficult.
Miccoli surgery (lumpectomy-assisted thyroid cancer surgery)
This procedure involves a small incision in the neck (usually 2 to 3 cm) and endoscopic-assisted removal of the thyroid. It is currently considered to be comparable to open surgery for papillary carcinoma without significant lymph node metastases. For lateral cervical zone lymph node dissection, it provides better visualization of zone IIA and IIB lymph nodes and can be done more smoothly relative to open surgery.
Patients who are concerned about large incisions that affect their appearance, have no more than 2 cm of maximum lateral cervical lymph node metastases, and have no lymph node fusion or extravasation may be considered first for the Miccoli procedure.
However, compared with open surgery, the lumpectomy-assisted technique does not fully expose the surgical site to the surgeon, so the surgeon still recommends open surgery for the following three conditions.
- Multiple lymph node metastases in the neck
- Significant tumor extravasation
- Local vascular adhesions
Robotic lumpectomy
The da Vinci robotic system is commonly used today, allowing the surgeon to operate in a three-dimensional, high-definition, magnified surgical view. It is more delicate and flexible than the manual hand, and also avoids manual chatter, offering unparalleled advantages of lumpectomy assistance and more stable and reliable operation. However, it is expensive and may cause tissue damage if operated inadvertently.
According to national guidelines, robotic laparoscopic surgery may be considered when the following conditions are met.
- The tumor is no larger than 2 cm in diameter; it does not invade adjacent organs such as the trachea, esophagus, or vascular nerves
- No extensive metastases in the cervical lymph nodes and no fusion and fixation of the enlarged lymph nodes
- No enlargement of the upper mediastinal lymph nodes
- The patient gave informed consent and had a strong cosmetic desire.
.
This procedure cannot be performed if:
- Has had surgery or radiation therapy to the neck
- Pregnant or breastfeeding women
- Short and flat neck, thoracic deformity, etc.
- Posterior sternal goiter
- Differentiated thyroid cancer with extrathyroidal invasion involving surrounding organs, extensive cervical lymph node metastasis or fusion and fixation of enlarged lymph nodes, metastatic lymph node cystic changes
- Metastatic lymph nodes greater than 2 cm in diameter, distant metastases, and dorsal thyroid tumor protruding beyond the thyroid peritoneum.
- Has severe coagulation disorders, cardiopulmonary dysfunction, and cannot tolerate general anesthesia and surgery
What are the possible risks of lumpectomy?
Complications of lumpectomy fall into two categories, one related to the thyroid surgery itself and the other to the lumpectomy technique. For the former, the risks of the lumpectomy technique are not significantly higher than those of open surgery. The latter mainly includes tumor residuals that may be caused by inadequate exposure and tumor implantation and metastasis caused by irregular operation. The surgeon will avoid these risks as much as possible by strictly grasping the indications for surgery and standardizing the operation.
Related reading:
Co-written by Dr. Tingting Zhang, Fudan University Cancer Hospital